
Recommended
More Related Content
Similar to PEN and amrs perspectives iprotocol.pptx
Similar to PEN and amrs perspectives iprotocol.pptx (20)
Recently uploaded
Recently uploaded (20)
PEN and amrs perspectives iprotocol.pptx
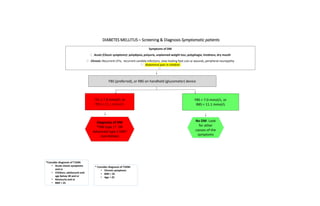
- 1. DIABETES MELLITUS – Screening & Diagnosis Symptomatic patients Symptoms of DM Acute (Classic symptoms): polydipsia, polyuria, unplanned weight loss, polyphagia, tiredness, dry mouth Chronic: Recurrent UTIs, recurrent candida infections, slow healing foot cuts or wounds, peripheral neuropathy Abdominal pain in children FBS (preferred), or RBS on handheld (glucometer) device FBS ≥ 7.0 mmol/L or RBS ≥ 11.1 mmol/L FBS < 7.0 mmol/L, or RBS < 11.1 mmol/L Diagnosis of DM *DM type 1? OR Advanced type 2 DM? (see below) No DM. Look for other causes of the symptoms *Consider diagnosis of T1DM: • Acute classic symptoms and or • Children, adolescent and age below 30 and or • Ketonuria and or • BMI < 25 * Consider diagnosis of T2DM: • Chronic symptoms • BMI > 25 • Age > 25
- 2. 2 Screen high risk patients • First degree (Parents and/or Siblings) family history of DM • Age (Above 40 years) • History of gestational DM • Hypertension • HIV Positive • Active TB • Obesity (BMI ≥ 30 kg/m²) • Cardiovascular disease (CVD): stroke, ischaemic heart disease, heart failure, peripheral artery disease • Chronic Kidney Disease (CKD): CrCl < 60 ml/min) FBS < 7.0* RBS < 11.1 FBS ≥ 7.0 RBS > 11.1 Repeat FBS within 1 week at facility Follow management cascade for confirmed T2DM FBS ≥ 7.0 Diabetes confirmed No DM Screening & Diagnosis of Asymptomatic Patients FBS or RBS on handheld device (glucometer) in mmol/L FBS 6.1 to 6.9 FBS 3.9 to 6.0 Impaired FBS • Dietary & lifestyle counseling • Re-screen after 6 months Refer to District Hospital • Dietary & lifestyle counseling • Re-screen after 1 year Discrepancy between 1st and 2nd test 3/6/2024
- 3. FBS >/= 7mmol/l to < 18mmol/l FBS> 18mmol/l Counsel on diet and physical activity Start metformin 500mg po bd Review in 1 month Test for urine ketones If ketones >/+ 2+ If ketones < 2+ Refer to hospital Check hydration status Dehydration present Dehydration absent Give IV fluids Start metformin 500mg po bb Glibenclamide 5mg po od Counsel on hypoglycemia Start metformin 500mg po bb Glibenclamide 5mg po od Counsel on hypoglycemia Re assess in 3 to 5 days If no improvement. Refer to Hospital If improved. Continue medication. Counsel on lifestyle Review after a month TREATMENT CASCADES FOR DIABETES MELLITUS Target not met from self monitoring or FBS> 7, RBS> 11.1 Target met from self monitoring or FBS < 7, RBS< 11.1 Check adherence Reinforce lifestyle changes Increase metformin to 1g bd Review in a month Continue with treatment Encourage self care Lifestyle counselling If target is met then continue with current medication If target id not met then add glibenclamide 5mg po od Review after a month If target is not met then refer to hospital
- 4. Systolic BP ≥140 or Diastolic BP ≥ 90 Stage 1 HTN SBP 140-159 or DBP 90-99 on 3 separate measurements over 2 weeks Stage 2 HTN SBP 160-179 or DBP 100-109 on 3 separate measurements over 1 week Stage 3 HTN SBP ≥ 180 or DBP ≥ 110 Hypertension patient education and counseling, Lab tests Begin medication Continue to monitor, adjust/add medication and follow up per protocol Prescribe diet and lifestyle management. Start treatment Patient education and counseling. Hypertension Diagnostic and Screening Cascade See diagnostic cascade for stage 3 HTN 3/6/2024 4 HTN only Begin medication AND REFER With: Stroke Heart Failure, Coronary artery disease persistent proteinuria High cholesterol With: DM or high *CVD Risk (2 or more of: smoking, obesity, sedentary lifestyle, high cholesterol) With: DM or high *CVD Risk (2 or more of: smoking, obesity, sedentary lifestyle, high cholesterol) With: Stroke Heart Failure, Coronary artery disease persistent proteinuria High cholesterol Begin medication AND REFER ←
- 5. BP still above target(140/90) despite good adherence: add Amlodipine 5 mg OD and manage according to Stage 2 hypertension flow chart START HCT 25 mg OD Reinforce lifestyle changes Review in 4 weeks BP ≥ 140/90 mmHg and <160/100mmHg • No diabetes mellitus • No cor-mobidities • Program Target: BP < 140/90 for ALL PATIENTS STAGE 1 HTN TREATMENT CASCADE Patients with HTN-only Preferred practice if resources permit • Offer counselling on Lifestyle(Diet and exercise) including: • Low salt diet • Regular exercises (minimum 30 min/day for 5-7 days per week of moderate intensity exercises) • No smoking • Aim for weight reduction to achieve BMI < 25 • Reduce alcohol intake • Low fat intake 3/6/2024
- 6. If BP still above target: confirm adherence and add AMLODIPINE 5 mg OD. Review in 4 weeks START Enalapril 10mg OD and refer. Review in 4 weeks 6 If BP still above target : confirm adherence and increase AMLODIPINE to 10 mg OD. Review in 4 weeks STAGE 1 HTN TREATMENT CASCADE PATIENTS WITH DM OR HIGH CVD RISK Refer BP ≥ 140/90 mmHg AND < 160/100 • Ideal target BP for DM-HTN: <130/80mmHg 3/6/2024 If BP still above target, Increase Enalapril to 20mg BD Review in 4 weeks • Offer counselling, educational session and prescribe lifestyle management including: • Low salt diet • Regular exercises (minimum 30 min/day for 5-7 days per week of moderate intensity exercises) • Stop smoking • Aim for weight reduction to chive BMI < 25 • Reduce alcohol • Reduce fat
- 7. If BP still above target despite adherence: increase AMLODIPINE to 10 mg OD. Review in 2 – 4 weeks If BP still above target: confirm adherence and add ENALAPRIL 10 mg OD. Review in 4 weeks If BP still above target: confirm adherence and increase ENALAPRIL to 20 mg OD or 20 mg OD. Review in 4 weeks If BP still above target : confirm adherence and consider start of SPIRONOLACTONE or ATENOLOL START HCT 25 mg OD AND Amlodipine 5 mg OD Review in 2 – 4 weeks 7 BP ≥ 160-179/100 -109 mmHg AND < 180/110 • Start treatment • Target: BP < 140/90 FOR ALL PATIENTS SECONDARY CARE LEVEL STAGE 2 HTN TREATMENT CASCADE If BP still above target: confirm adherence and increase ENALAPRIL to 40 mg OD Review in 4 weeks If BP still above target despite adherence: Refer
- 8. 8 HTN Stage 3 SBP ≥ 180 and/or DBP ≥ 110 Known hypertensive: Reinstitute/ intensify oral medication and Refer Hypertensive emergency: Marked confirmed elevated BP with symptoms and signs indicative of impairment of one or more organ systems (brain, eyes, heart, aorta, or kidneys) Start HCT 25 mg and Amlodipine 5 mg and refer urgently to hospital Hypertensive urgency: Marked confirmed elevated BP but no damage to the body's organs (stable patient) New hypertensive: Start HCT 25 mg and Amlodipine 5 mg and Refer Signs & symptoms: pale & cool skin, sweating, fatigue, very fast or very slow pulse, SOB, headache, confusion, acute chest pain, seizure, body swelling Target organ damage Signs & symptoms? New/progressive/ worsening? STAGE 3 HTN TREATMENT CASCADE NO YES Review patients after 3 days. If follow up BP < 180/110 titrate medication upwards and encourage review with the doctor. If persistently high, emphasize need for referral! 3/6/2024
- 9. Referal criteria • BP >180/>110 mm Hg (urgent referral) • BP ≥140 or ≥ 90 mmHg in people < 30 yrs (to exclude secondary hypertension) • Known heart disease, stroke, transient ischemic attack, DM, kidney disease (for assessment, if this has not been done) • New chest pain or change in severity of angina or symptoms of stroke • Raised BP ≥140/90 ( in DM above 130/ 80mmHg) while on treatment with 2 medications • Any proteinuria • Newly diagnosed DM with urine ketones 2+ or in lean persons of <30 years • DM with poor control despite maximal metformin with sulphonylurea • DM with severe infection and/or foot ulcers • DM patients with glucometer reading above 18mmol/l • DM with recent deterioration of vision or no eye exam in 2 years • High cardiovascular risk
- 10. SEVERE HYPOGLYCAEMIA OR SIGNS (plasma glucose < 2.8 mmol/L) If conscious, give a sugar-sweetened drink If unconscious, give 20–50 ml of 50% glucose (dextrose) IV over 1–3 minutes SEVERE HYPERGLYCAEMIA OR SIGNS AND SYMPTOMS (plasma glucose > 18 mmol/L and urine ketone 2+) Set up intravenous drip 0.9% NaCl 1 litre in 2 hours; continue at 1 litre every 4 hours REFER to hospital MANAGEMENT OF ACUTE COMPLICATIONS
Editor's Notes
- Key for abbreviations needed.
- Monitoring serum K and Creatinine is recommended after 2-4 weeks of adding enalapril (or spironolactone) or adjusting enalapril dose