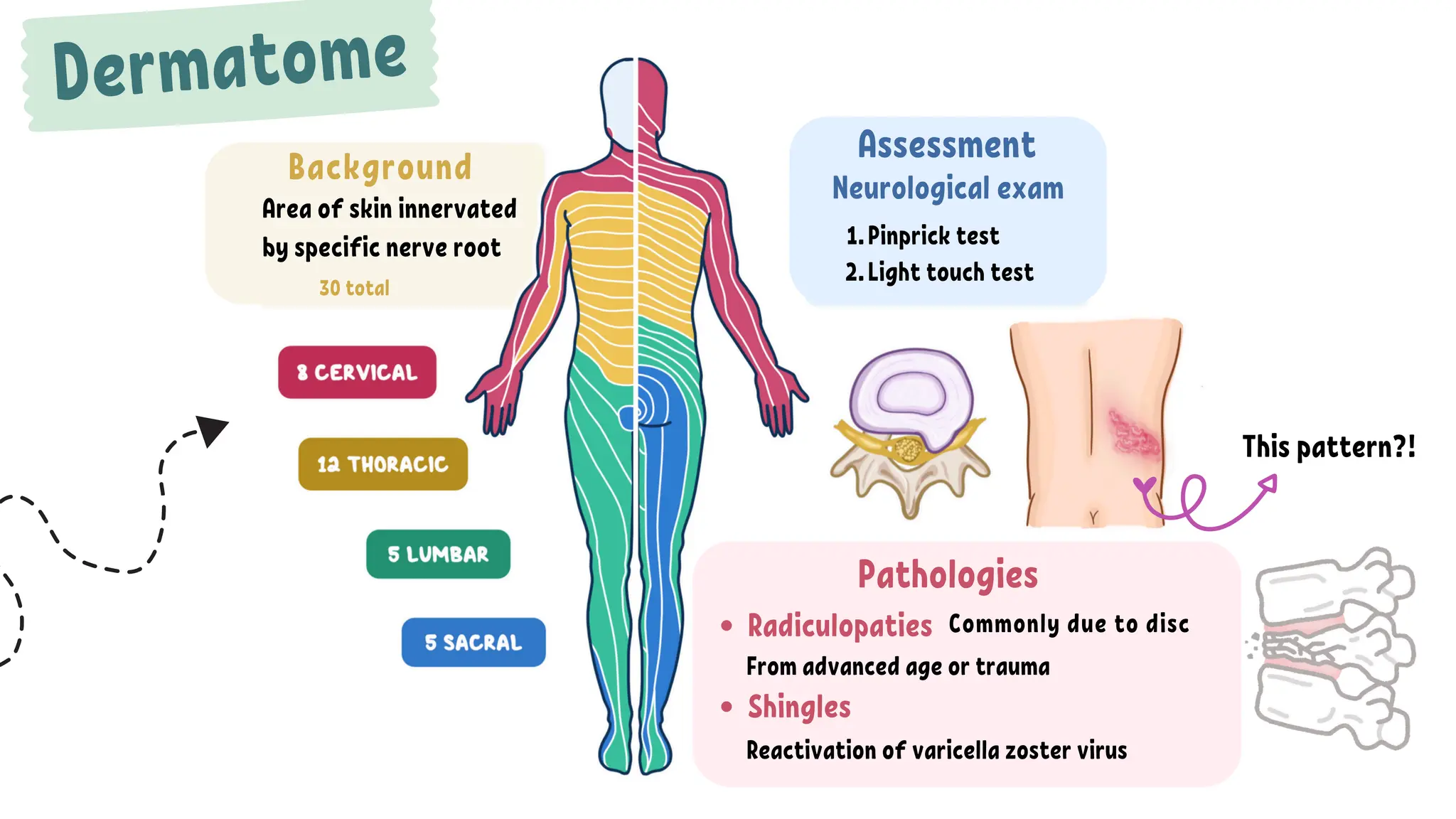
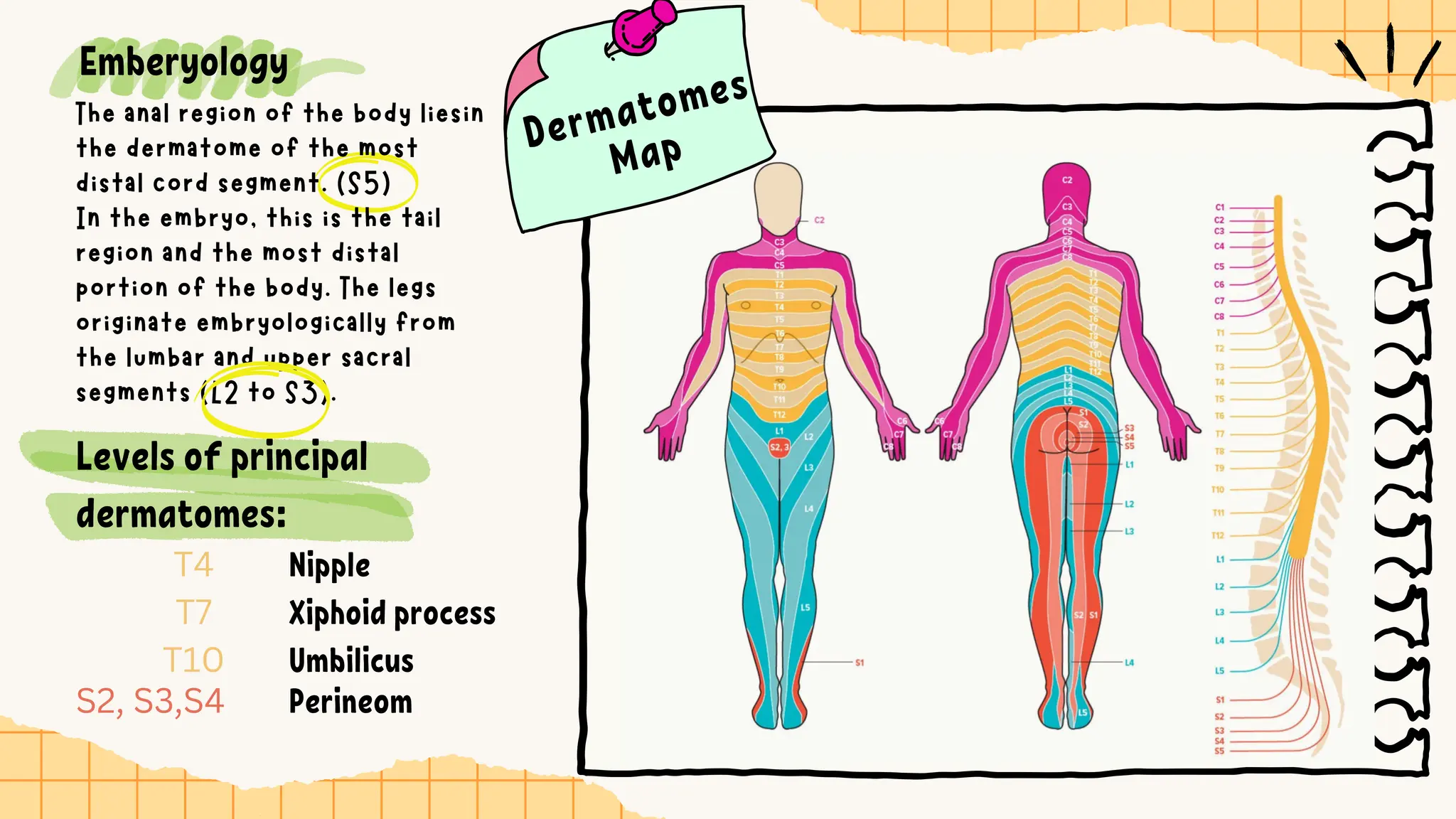
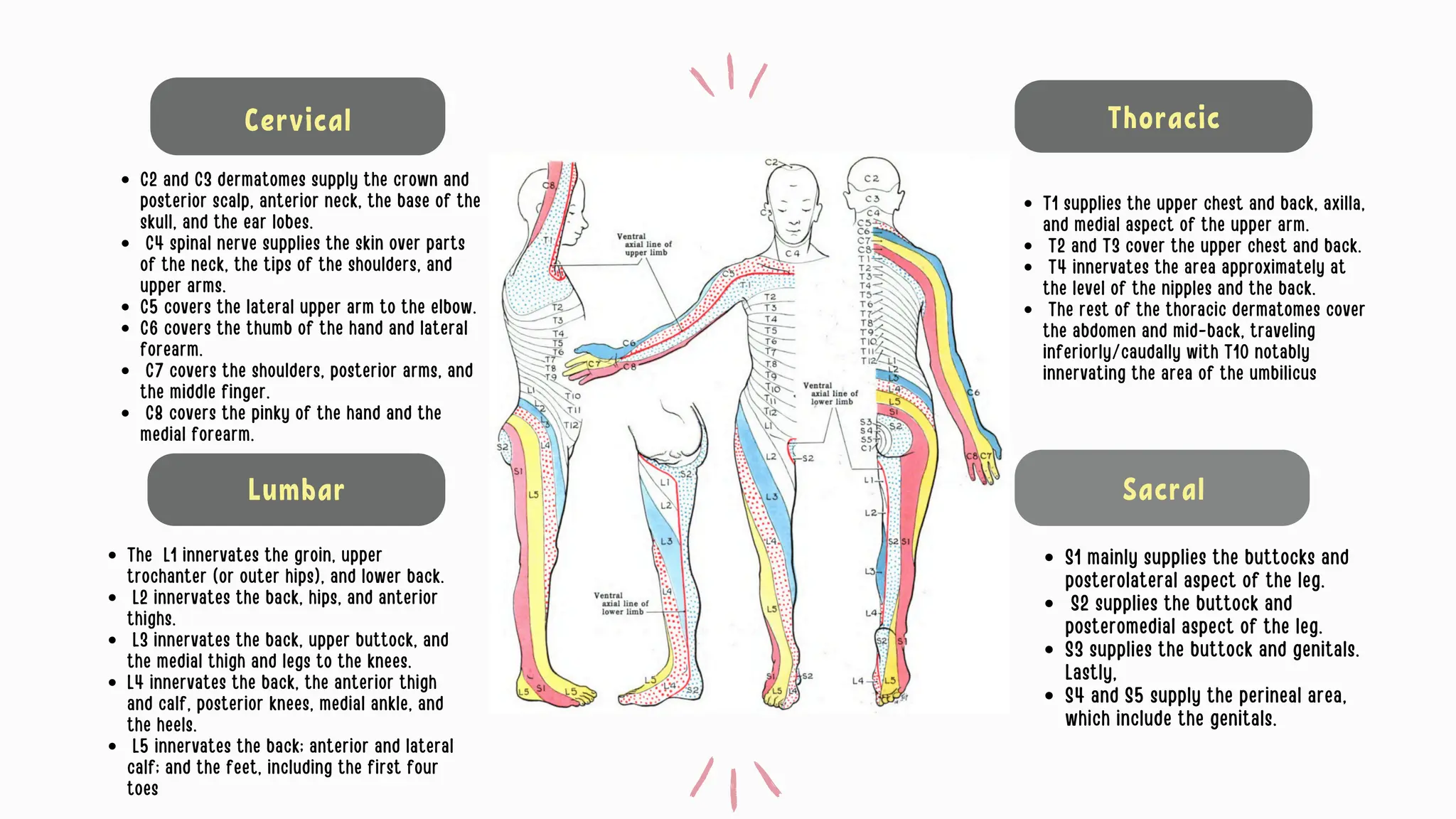
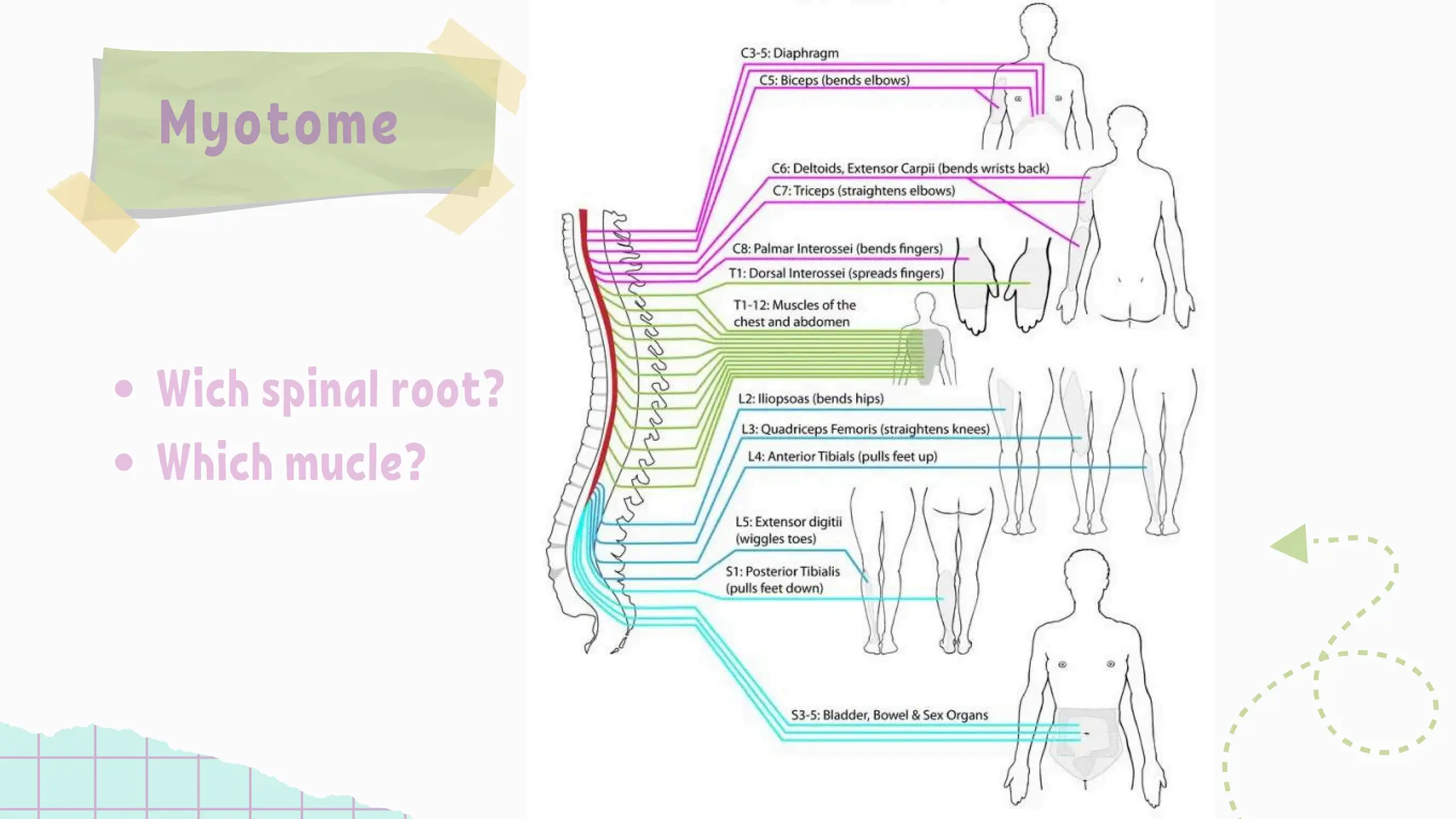
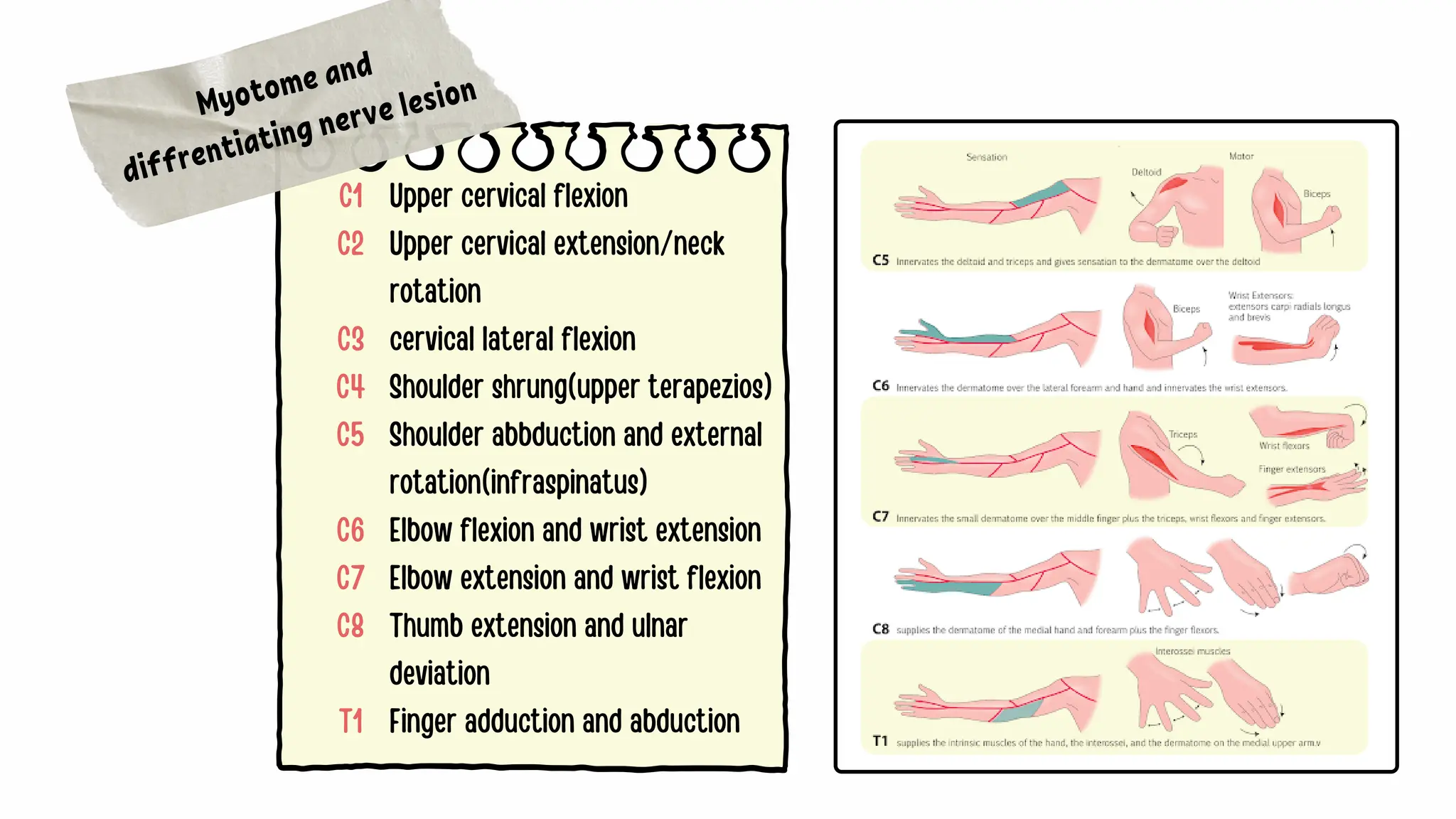
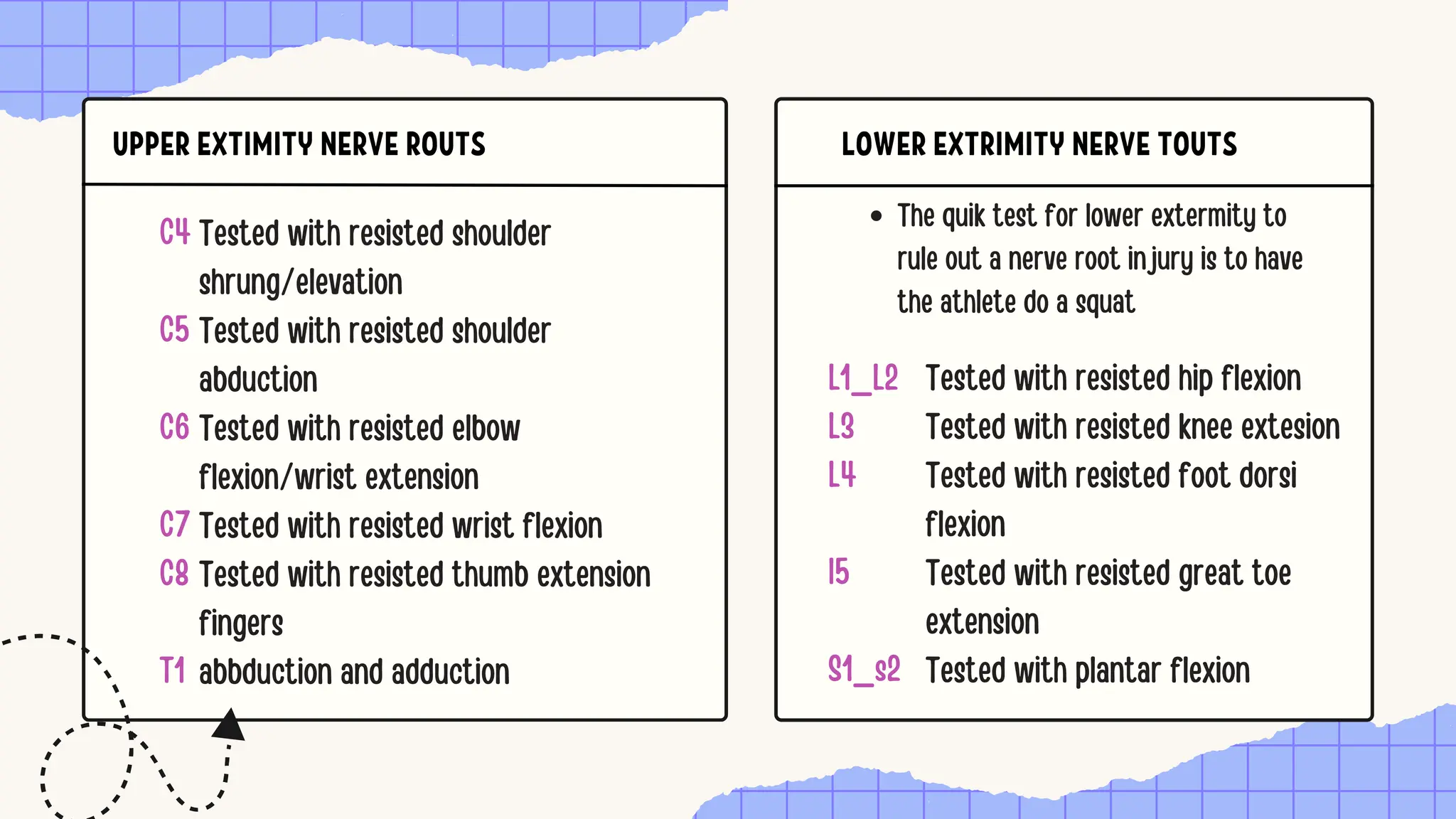
The document discusses the significance of dermatomes and myotomes, detailing the specific areas of skin and muscles innervated by spinal nerve roots. It outlines the various dermatomes associated with different spinal levels and provides clinical insights into muscle weaknesses related to specific nerve root lesions. Additionally, it includes assessment techniques for evaluating nerve root injuries in the upper and lower extremities.










![1. brachial plexus & its applied anatomy[1]](https://cdn.slidesharecdn.com/ss_thumbnails/1-brachialplexusitsappliedanatomy1-100602035429-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)


























































