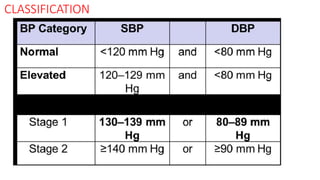
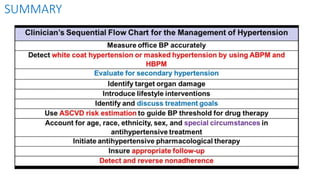
1) The 2017 ACC/AHA Guideline provides recommendations for the prevention, detection, evaluation, and management of high blood pressure in adults. It establishes new normal and elevated blood pressure categories and treatment thresholds.
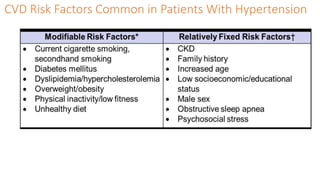
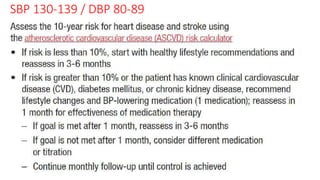
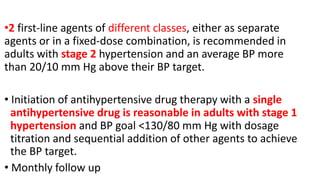
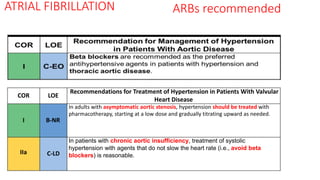
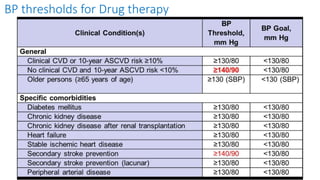
2) Key recommendations include treating stage 1 hypertension with nonpharmacological therapy and initiating drug treatment for those with a 10-year CVD risk over 10%; treating stage 2 hypertension with nonpharmacological therapy and drug treatment; and treating hypertension in patients with diabetes, CKD, heart disease, and other conditions.
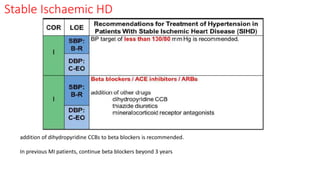
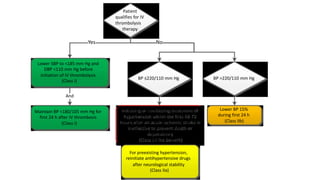
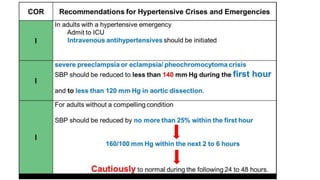
3) Treatment involves initiating antihypertensive drug therapy with lifestyle modifications and titrating medications to achieve a blood pressure target of less than 130/80 mm Hg for most patients.