Downloaded 29 times

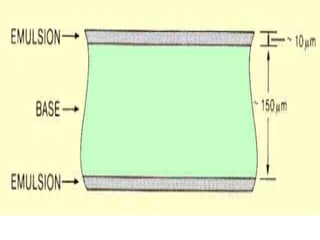

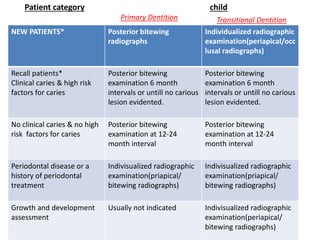
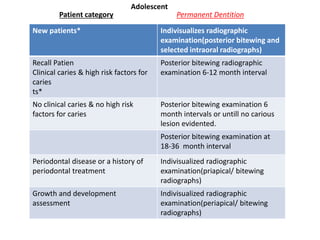


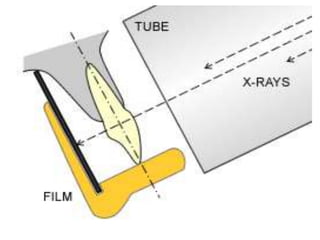
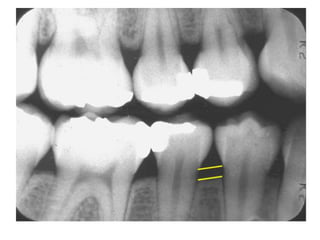
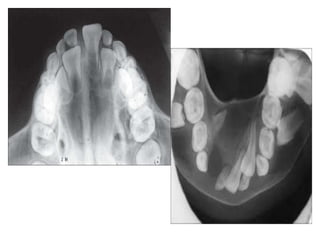
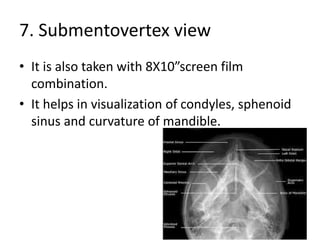
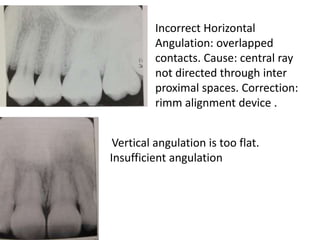
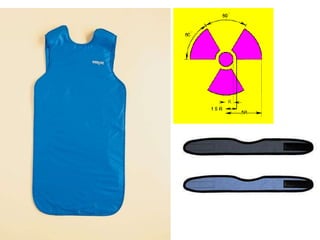


This document provides an overview of pediatric radiology. It discusses the composition of radiographic films and the different types of radiographs used in pediatric dentistry, including intraoral and extraoral films. Intraoral films include periapical, bitewing, and occlusal radiographs. Extraoral films and specialized imaging techniques like panoramic radiography are also covered. The document outlines patient selection criteria and guidelines for prescribing radiographs. It discusses technical errors and emphasizes principles of radiation safety, including justification of exposures and methods for patient, personnel, and public protection.




















































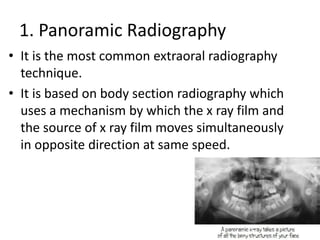
![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)














