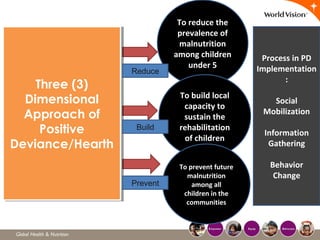
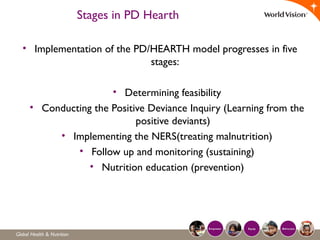
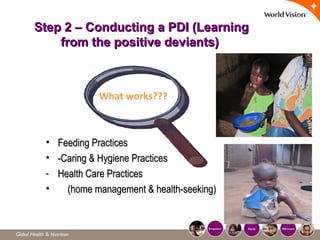
The document discusses the Positive Deviance Hearth Nutrition Model. It begins by defining positive deviance as behaviors that depart from norms in a positive way. The model looks for solutions within communities rather than what is missing. A Positive Deviance Inquiry identifies behaviors of positively deviant community members that enable better nutrition. Hearth sessions then promote these behaviors over 12 days to rehabilitate malnourished children while empowering communities. The multi-step process emphasizes identifying indigenous solutions, community participation, affordability, and sustainability.