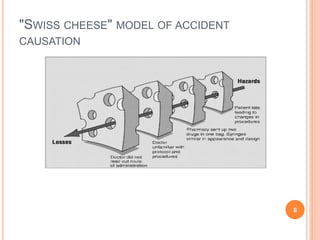
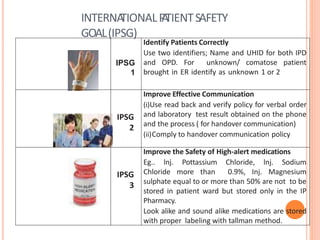
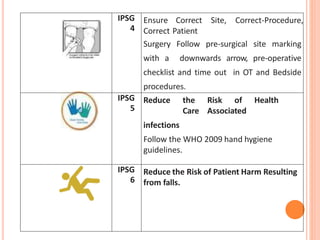
This document discusses patient safety and medical errors. It defines key terms like adverse events, near misses, and sentinel events. Errors can be caused by active failures from individuals or latent system issues. The Swiss cheese model of accident causation illustrates how multiple factors can align to cause harm. A just culture approach examines systems instead of blaming individuals. International patient safety goals aim to reduce errors through practices like proper patient identification and hand hygiene. Communication failures and lack of labeling contributed to a case where epinephrine was given instead of saline. Overall, patient safety requires a systems approach rather than blaming individuals.