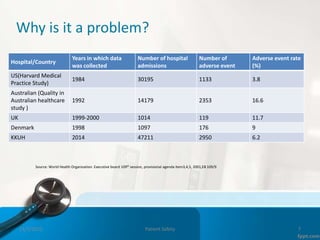
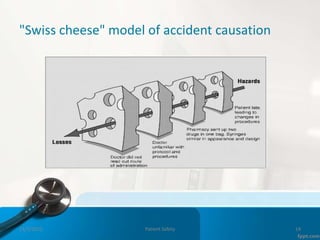
This document provides an introduction to patient safety. It defines patient safety as the reduction of unnecessary harm from healthcare. Significant numbers of patients are harmed or die each year from medical errors. The six key dimensions of healthcare quality are discussed, including being safe, effective, efficient, equal, timely, and family-centered. Sources of error include active human errors and latent system errors. A just culture focuses on system flaws rather than individual blame. Clinical incidents encompass adverse events, near misses, and sentinel events. Maintaining safety involves adhering to best practices around issues like hand hygiene, medication reconciliation and falls prevention.











































































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)





