Downloaded 426 times
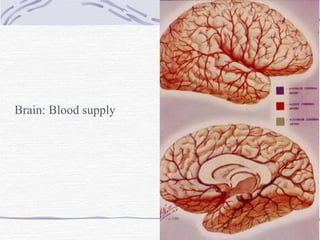
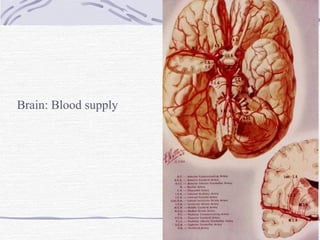
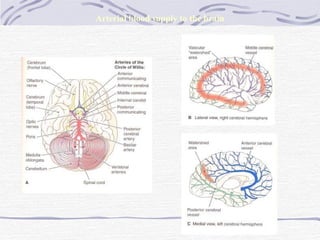
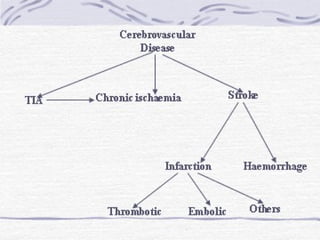
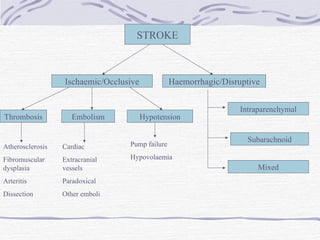
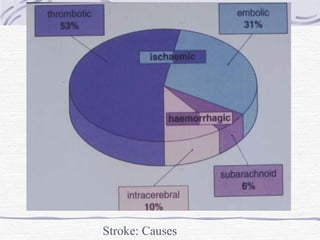
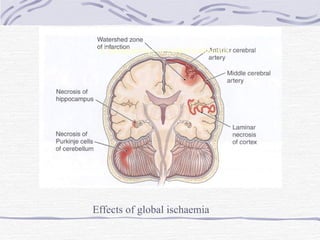
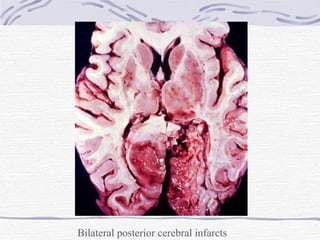
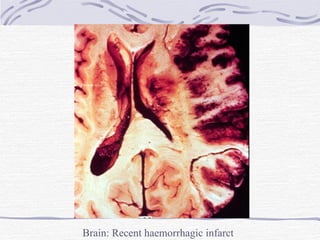
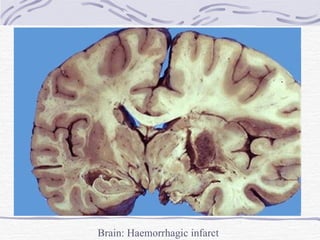
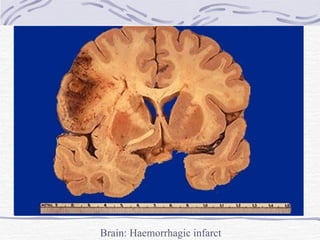
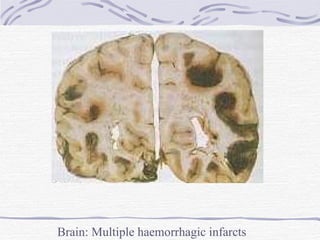
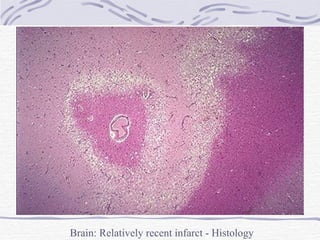
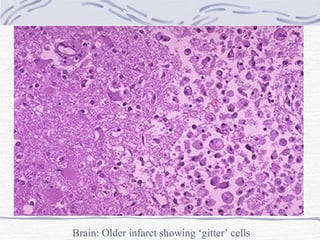

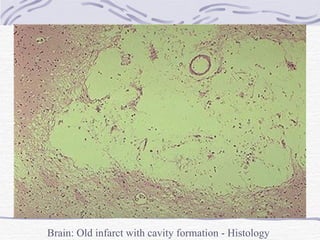
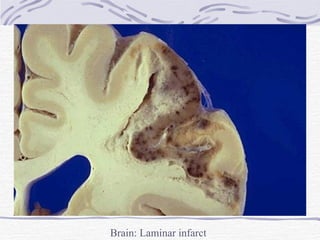
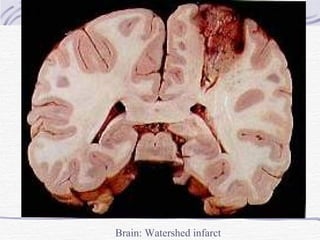
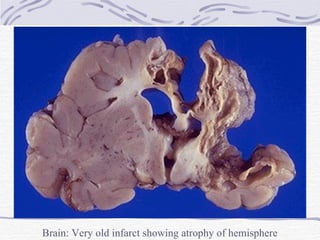
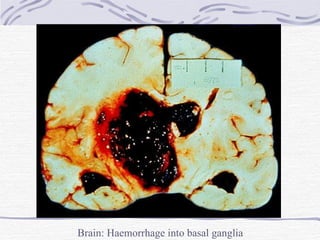
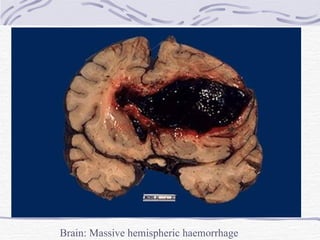
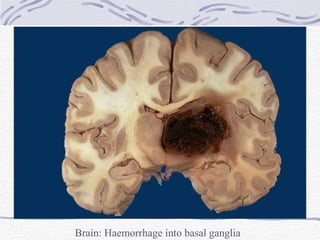
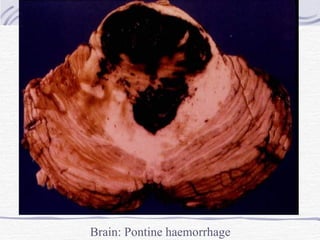
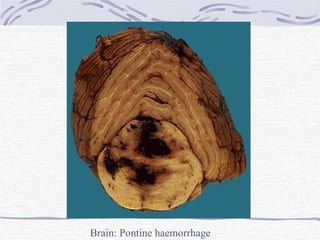
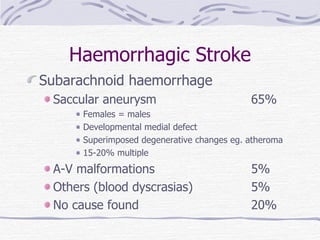
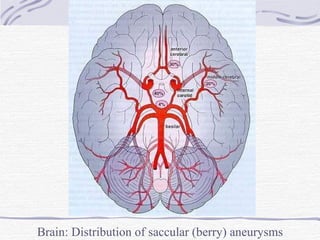
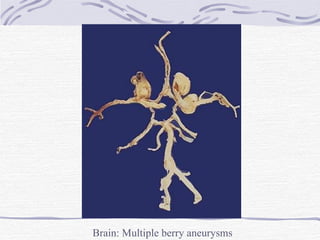
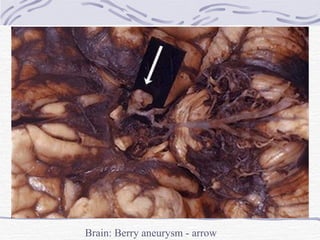
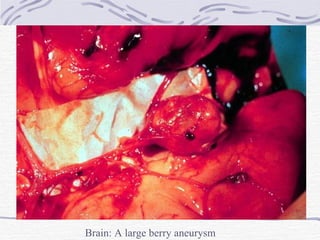
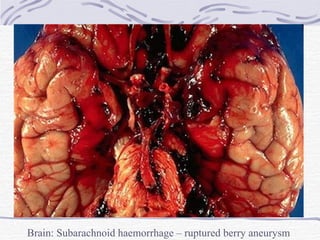
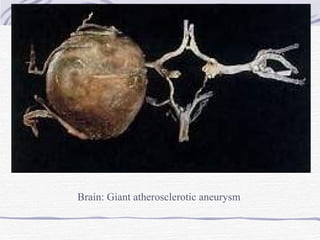
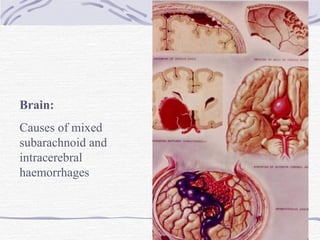
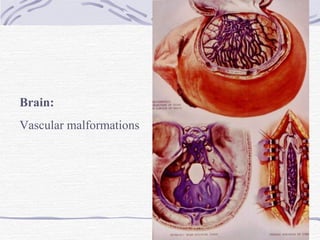
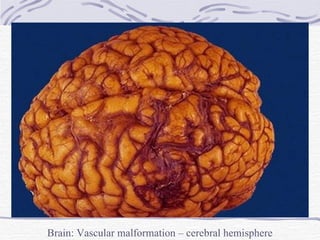
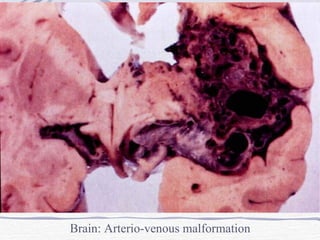
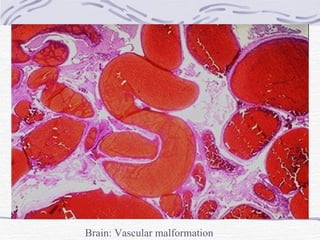

This document summarizes pathology related to cerebrovascular disease. It discusses different types of strokes including ischemic, hemorrhagic, and transient ischemic attacks. Specific factors that can contribute to tissue damage in ischemic strokes are explained. Locations and appearances of infarcts over time are described. Causes and presentations of hemorrhagic strokes including those from aneurysms and arteriovenous malformations are covered.





























































![Stroke [uncensored] - by MHR Corporation](https://cdn.slidesharecdn.com/ss_thumbnails/mhr4-stroke-101129110104-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)

























