Downloaded 385 times

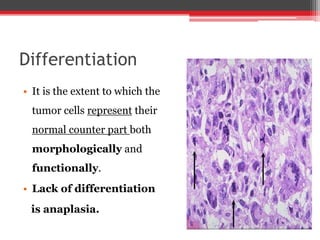
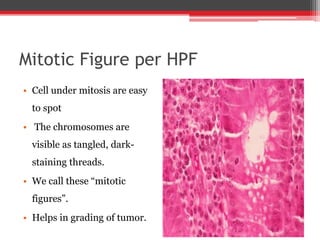
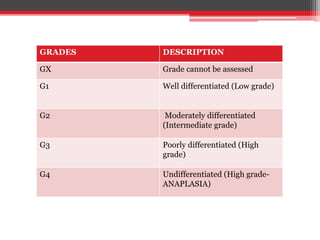
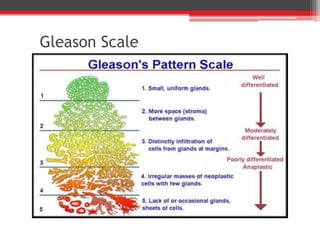
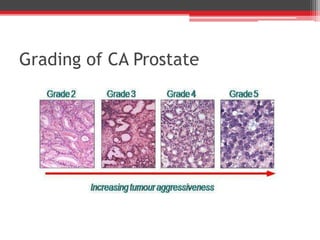


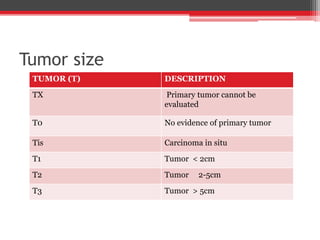
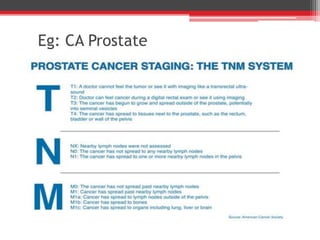
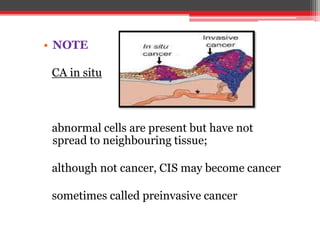
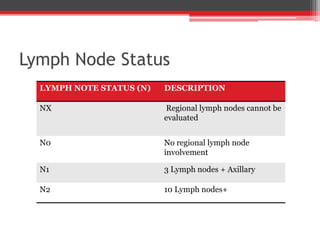
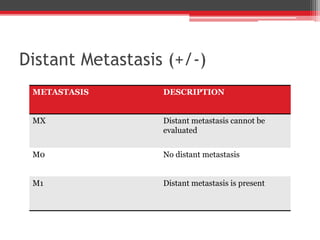
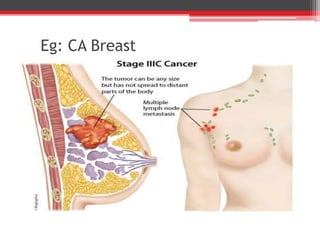
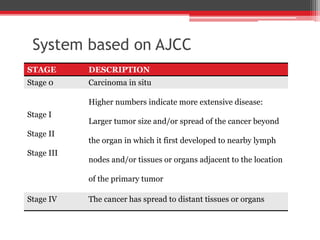
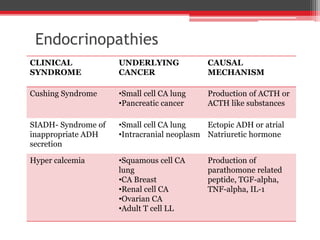
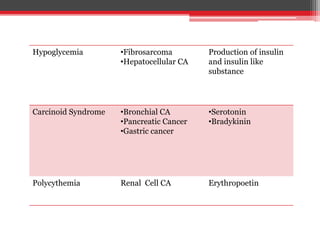
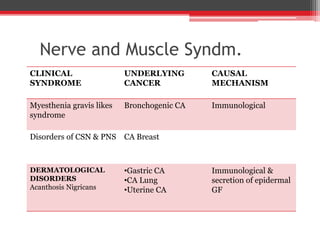
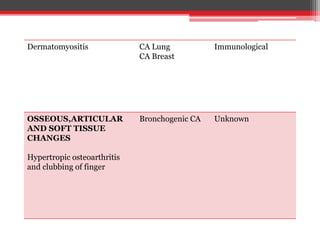
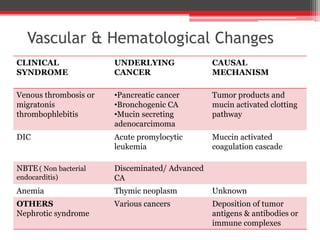

This document discusses grading and staging of tumors and paraneoplastic syndrome. Grading is done based on differentiation and mitotic figures, with tumors graded on a scale of G1 to G4. Staging uses the TNM system to describe tumor size (T), lymph node involvement (N), and metastasis (M). Together, grading and staging provide information on prognosis and guide treatment. Paraneoplastic syndromes are unrelated to direct tumor involvement and may be caused by hormones or antibodies. Examples include endocrinopathies, neurological disorders, dermatological changes, and vascular/hematological syndromes associated with certain cancers. Grading, staging, and recognizing paraneoplastic syndromes help characterize cancers and their systemic














































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)














