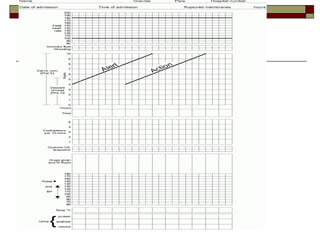
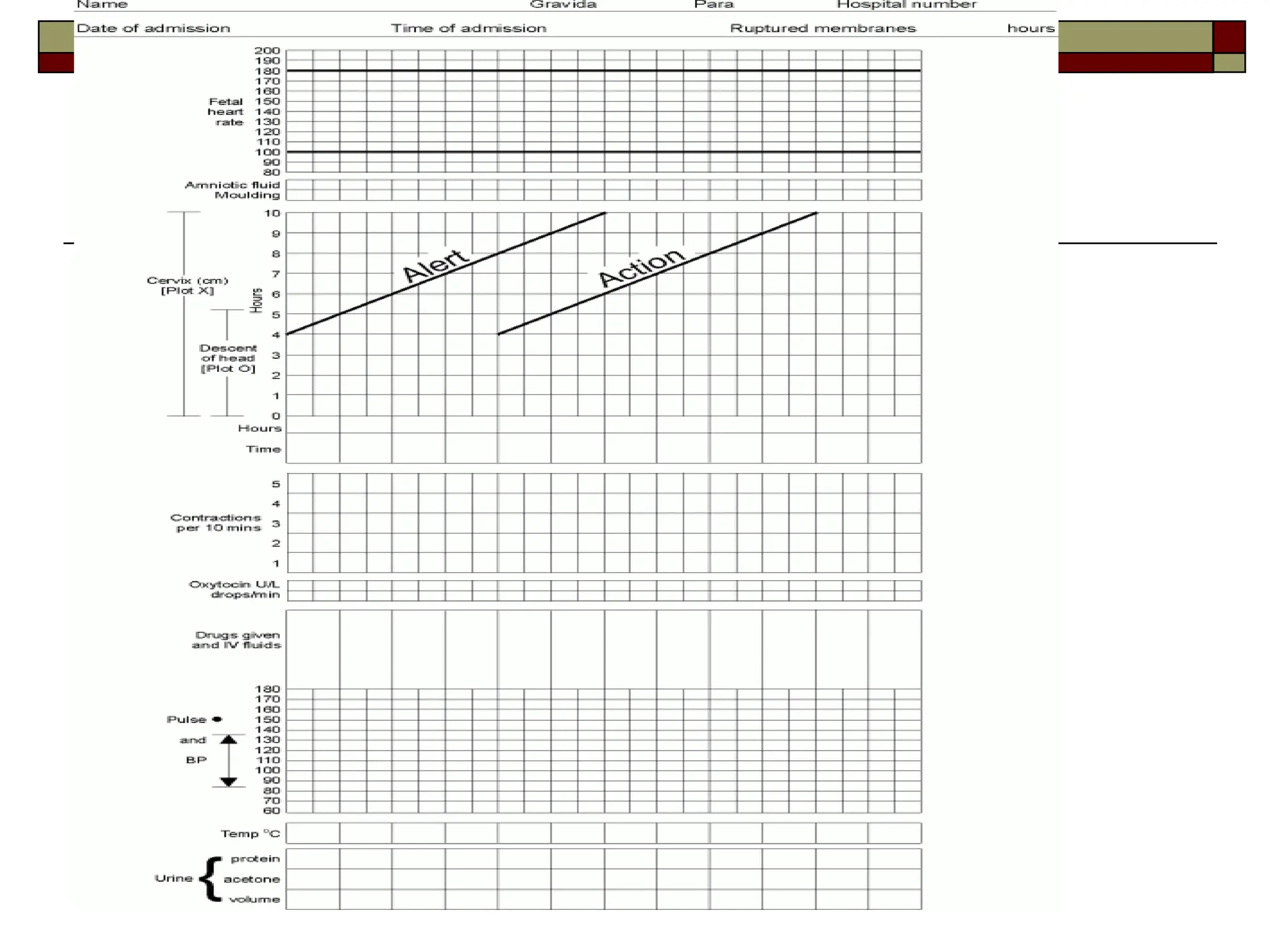
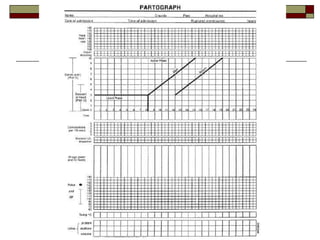
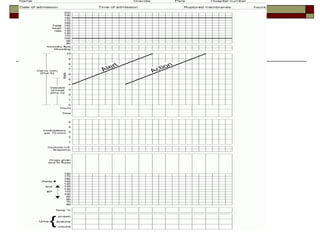
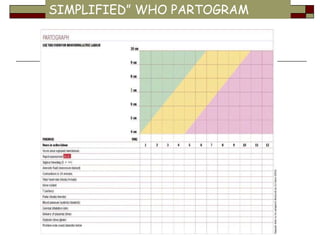
The document outlines the importance and protocols for using the WHO partogram in labor management, which is a graph designed to monitor labor progress and maternal and fetal well-being. It emphasizes early detection of abnormalities to prevent complications like obstructed labor, thereby reducing maternal and perinatal mortality. Specific guidelines for using the partogram in different health facilities and various special cases are also provided.

















































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

















