

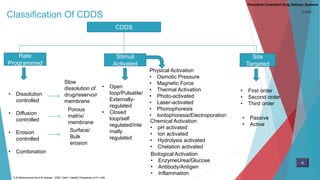
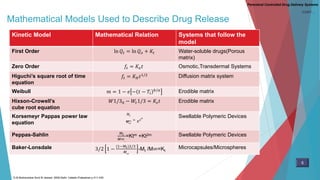
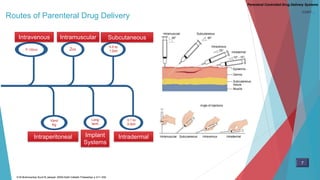











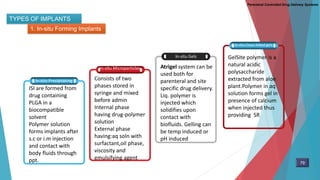
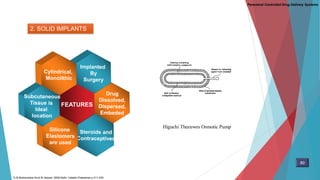
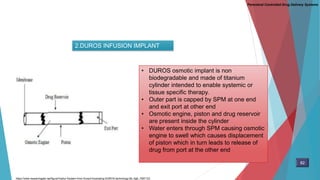
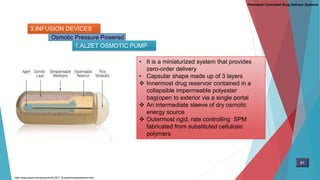


This document discusses various parenteral controlled drug delivery systems. It begins by defining controlled drug delivery and the need for parenteral controlled delivery systems. It then covers topics like classification of parenteral controlled delivery systems, approaches used, polymers employed, essential requirements, additives, mathematical models of drug release, injectables including solutions, resealed erythrocytes and various particle/implant systems. The document provides an overview of key concepts and considerations in parenteral controlled drug delivery.



































































