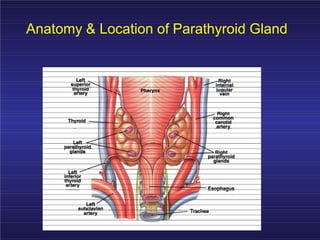
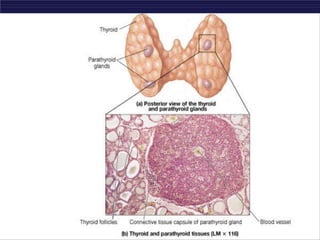
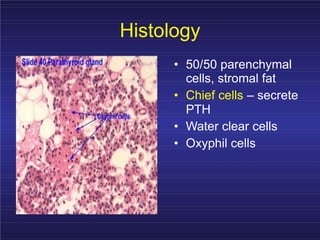
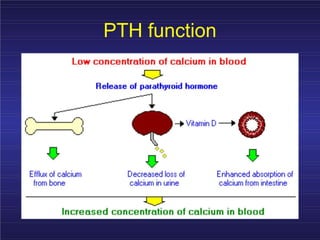
This document discusses disorders of the parathyroid glands. It covers the anatomy and function of the parathyroid glands, parathyroid hormone, and disorders involving abnormal parathyroid function such as hyperparathyroidism and hypoparathyroidism. Hyperparathyroidism can be primary, secondary, or tertiary and involves excessive PTH production leading to hypercalcemia. Hypoparathyroidism is a deficiency of PTH causing hypocalcemia. Surgical removal of the parathyroid glands can cause hypoparathyroidism as a complication.