Transport & metabolismof thyroid hormones
T 4 and T3 are relatively lipophilic, their free forms in plasma are
in equilibrium with a much larger pool of protein-bound thyroid
hormones in plasma.
Protein binding:
Maintains large pool of hormone that can readily be mobilized
as needed.
Prevents excess uptake by the first cells encountered and
promotes uniform tissue distribution
The plasma proteins that bind thyroid hormones are Albumin,
Transthyretin (Thyroxine-binding Prealbumin) and Thyroxine-
Binding Globulin (TBG).
8.
Transport & metabolismof thyroid hormones
.
Deiodination of T 4
to produce T3
Deiodinase activity varies among different tissues & at different
periods.
Thyroid hormones enter cells and act by binding to nuclear
receptors.T is 3-5 times more potent thanT . RT is inert.3 4 3
Hormone Total plasma level Free hormone level
T4 8 μg/dL 2 ng/dL (0.02%)
T3 0.15 μg/dL 0.3 ng/dL (0.2%)
Causes of permanentCH
Thyroid dysgenesis
Defects in thyroid hormone synthesis and
secretion (Thyroid dyshormonogenesis)
TSH resistance
Central (hypothalamic–pituitary)
hypothyroidism
20.
Causes of transientCH
Antithyroid drugs
Iodine excess.
Worldwide, iodine deficiency
Transient hypothyroxinemia of prematurity
TSH receptor-blocking IgG antibodies
Large liver hemangiomas
21.
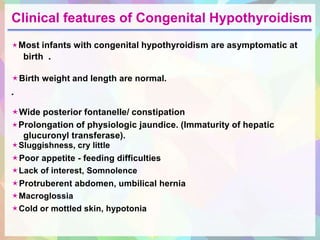
Clinical features ofCongenital Hypothyroidism
Most infants with congenital hypothyroidism are asymptomatic at
birth .
Birth weight and length are normal.
.
Wide posterior fontanelle/ constipation
Prolongation of physiologic jaundice. (Immaturity of hepatic
glucuronyl transferase).
Sluggishness, cry little
Poor appetite - feeding difficulties
Lack of interest, Somnolence
Protruberent abdomen, umbilical hernia
Macroglossia
Cold or mottled skin, hypotonia
22.
Clinical features ofCongenital Hypothyroidism
By 3-6 mo of age the clinical picture is fully developed, if
untreated.
The child’s growth will be stunted, the extremities are short,
and the head size is normal or even increased.
Coarse facial features: The eyes appear far apart, and the
bridge of the broad nose is depressed. The palpebral fissures
are narrow and the eyelids are swollen. The mouth is kept
open, and the thick, broad tongue protrudes.
Dentition will be delayed.
23.
Clinical features ofCongenital Hypothyroidism
Myxedema is manifested, particularly in the skin of the
eyelids, the back of the hands, and the external genitals.
Carotenemia can cause a yellow discoloration of the skin, but
the sclerae remain white.
Development is delayed.
Voice is hoarse.
Sexual maturation may be delayed.
Approach to anewborn with positive
screening test for Congenital Hypothyroidism
Positive screening test on filter paper sample
Serum T / Free T , TSH4 4
Normal Abnormal
Thyroid Scan
Normal EctopicAbsent Uptake
Ectopic Thyroid Gland
START
TREATMENT -
DON’T WAIT
FOR SCAN
26.
Approach to anewborn with positive
screening test for Congenital Hypothyroidism
Abnormal T , TSH & Normal Thyroid Scan4
Tg (Thyroglobulin) measurement
Normal Absent
Tg synthetic defect
Transient
congenital
hypothyroidism
Thyroid hormone
synthetic defect
or drug effect
TBII (Thyroid Binding Inhibitory
Immunoglobulin) measurement
Positive Negative
27.
Approach to anewborn with positive
screening test for Congenital Hypothyroidism
Abnormal T , TSH & Absent uptake on Thyroid Scan4
Ultrasound
Normal gland No thyroid tissue
Thyroid agenesis
TSH receptor or
Thyroid hormone
biosynthetic defect
Transient
congenital
hypothyroidism
TBII (Thyroid Binding Inhibitory
Immunoglobulin) measurement
Positive Negative
28.
Treatment of congenitalhypothyroidism
Infants with low T4 and elevated TSH should be started on L-
Thyroxine as soon as the diagnosis is made.
Initial dose of L-Thyroxine is 10-15 μg/Kg/day.
Daily dose should be crushed and placed directly on the tongue
in the morning.
If a dose is missed, then double dose should be given on the
next day.
29.
Treatment of congenitalhypothyroidism
Goal of therapy: T4 should be kept in the upper half of normal range
with the TSH
suppressed in the normal range.
It takes less than a week for T
normalize.
4 to rise and 4-5 weeks for TSH to
Monitoring: T4 and TSH should be monitored according to following
schedule.
Growth and development of infant should be monitored.
:
0 to 6 months Every 6 weeks
6 months to 3 years Every 3 months
Beyond 3 years Every 6 months
6 to 8 weeks after any dose change.
30.
Neonatal Screening Programme
•Dried blood sample after 72 hrs of life/ cord
blood
• T4/ TSH
• Appropriate cut offs of TSH should be used
31.
Acquired Hypothyroidism
• Etiology
1.Autoimmune Thyroiditis- most common cause
2. Iodine Deficiency
3. Goitrogens
4. Secondary hypothyroidism
• F> M
• Goiter
• Association with other autoimmune condition
32.
Evaluation
• Proper familyhistory
• Examination : type of goiter
• Thyroid function tests
• Anti TPO( thyroid peroxidase)
• MRI brain
• Bone age
33.
Clinical features
• Subtle
•Short stature
• Cold intolerance, lethargy, constipation
• Delay in dentition
• Poor school performance
• Delayed puberty
• Goiter
All children with unexplained
developmental delay, mental
sub normality and short
stature should be evaluated
for hypothyroidism
34.
Management
• L- Thyroxine
•Dose is 100 ug/m2
• Gradual build of dose
• Empty stomach
• Follow up 3-6 monthly
• Maintain TSH in normal range
• Mostly life long therapy
35.
Goiter
• Enlargement ofThyroid gland
• Thyromegaly- when lateral lobe of thyroid is
larger than the distal phalanx of child`s thumb
Estimation of thyroid size by palpation( WHO)
Stage 0 No goiter
1 A Goiter detectable only by palpation
1 B Palpable, visible when neck is fully extended
2 Goiter visible in normal neck position
3 Very large goiter, recognized from distance
36.
Etiology( Goiter)
• Maybe associated with decreased, increased or
normal thyroid function
• Hypothyroidism- any cause except dysgenesis
• Iodine deficiency
• Infiltration( autoimmune,neoplasm,
hemochromatosis)
• Grave`s disease( TSH receptor stimulating
antibodies)
• Congenital
37.
• Diffuse vsNodular goiter
• Acute painful goiter
• Investigations-
thyroid function test
Anti TPO
USG
FNAC
Iodine Deficiency Disorders(IDD)
• Endemic Goiter
- Iodine deficiency prevalent
- endemic goiter is present when the
prevalence of goiter in a defined population
exceeds 5 %
- TSH increased, Low T3, T4
- Iodine supplementation
- Epidemiological measures
40.
• Endemic Cretinism
-endemic goiter, severe iodine def
- clinical features
deaf- mutism
squint
mental retardation
spastic/ rigid neuromotor disorder
short staure
coarse facial features
• Neurological cretinism
• Myxedematous cretinism
41.
National Iodine DeficiencyDisorder
control Programme(NIDDCP) 1992
• To reduce the burden of iodine deficiency to <10 %
among adults and < 5% among children
• Promotion of iodised salt
• Surviellance
• RDA of iodine – 40-120 ug for children upto 10 yrs
- 150 ug for older children and adults
- additional 25 ug during pregnancy
- additional 50 ug during lactation
• Iodination of salt- 1 part/ 25000 to 50000 parts of salt
43.
• 1. atwo year old child presented to the opd
with history of short stature, tiredness,
constipation. Examination revealed a palpable
goiter. Serum T4 decreased, TSH increased.
Most probable diagnosis
a) thyroid dysgenesis
b) thyroid dyshormonogenesis
c) TSH receptor blocking antibody
d) central hypothyroidism
44.
• 2. A14 year old female has thyroid enlargement,
firm, non tender, nodular. T 4= 5.2( normal), TSH
= 17.5 mIU/l . Most likely diagnosis
a) acute suppurative thyroiditis
b) Graves disease
c) Hashimoto thyroiditis
d) Simple colloid goiter
e) solitary thyroid nodule