The document provides an overview of pain pathways and physiology. It discusses:
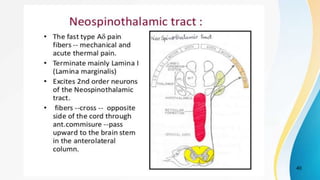
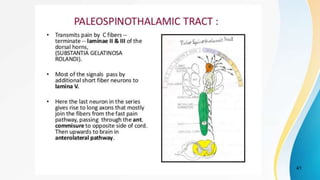
- The dual pain pathway in the spinal cord and brainstem, including the neospinothalamic and paleospinothalamic tracts.
- Pain receptor types and the chemicals involved in mediating pain.
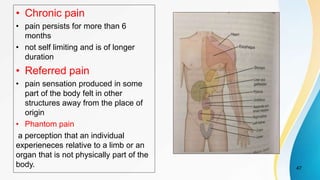
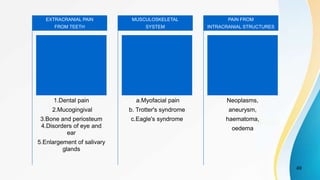
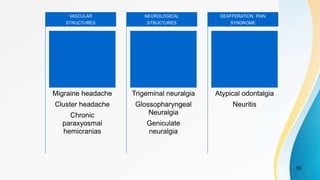
- Classification of different types of pain including somatic, visceral, acute, chronic, referred, and phantom pain.
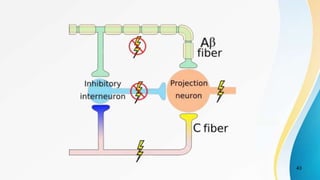
- Theories of pain transmission including specificity theory and gate control theory.
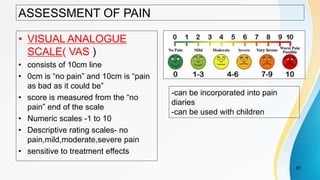
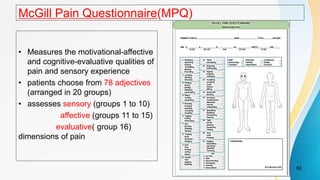
- Assessment tools for pain such as visual analogue scales and McGill Pain Questionnaire.

































![Face nerve &_vessels_(2)_(0)[1]](https://cdn.slidesharecdn.com/ss_thumbnails/facenervevessels201-170504173920-thumbnail.jpg?width=640&height=640&fit=bounds)










































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



