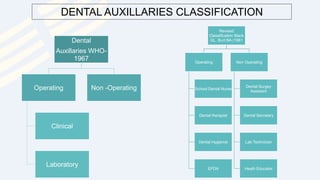
This document provides an overview of dental manpower in India, including the roles of dentists and different types of dental auxiliaries. It discusses the qualifications and duties of dentists and defines dental auxiliaries as technical workers who assist dentists. The document outlines several categories of dental auxiliaries in India, such as dental surgeons, therapists, hygienists, and laboratory technicians, and describes their training requirements and responsibilities. It also introduces concepts like four-handed and six-handed dentistry which utilize dental auxiliaries to improve treatment efficiency.






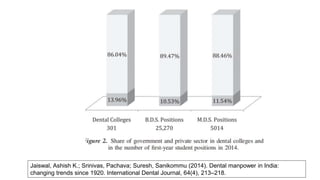
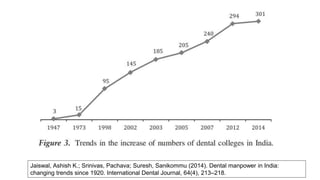
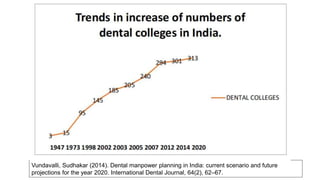
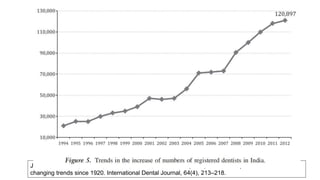



















![Tools of dental_public_health[1]](https://cdn.slidesharecdn.com/ss_thumbnails/toolsofdentalpublichealth1-151108134342-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)





















































