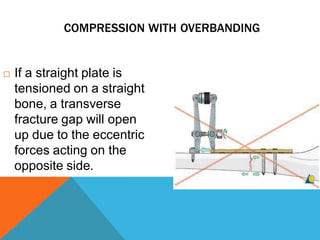
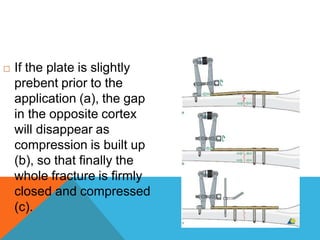
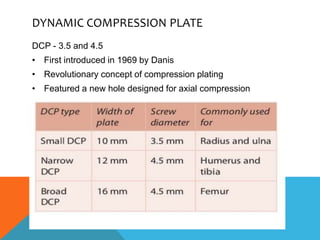
The document outlines the principles and history of orthopedic plates used for internal fixation of bone fractures, established by the AO in 1958. It discusses various types of plates, including dynamic compression plates, condylar plates, and reconstruction plates, along with their mechanical functions and clinical applications. The importance of proper plate design, length, and the principles of stress and strain in relation to bone healing and fixation are also highlighted.