Downloaded 273 times



















































The document discusses outpatient departments (OPDs) in hospitals. It defines an OPD and provides reasons for their establishment, including rising healthcare costs and limited hospital beds. OPDs provide about 30-35% of hospital revenue. Key points made include: - OPDs see over 50% of inpatients and act as screening points for treatment need. On average, 500 outpatients are seen per hospital bed per year. - Common problems faced by OPDs include insufficient doctors and facilities, long wait times, and lack of privacy. Queuing theory principles and appointment systems can help minimize wait times. - Proper design, staffing, equipment and management of patient flow are needed to improve OPD efficiency
Introduction of Colonel Zulfiquer and credentials in health services.
Defines OPD, highlights its significance in healthcare, and mentions economic factors.
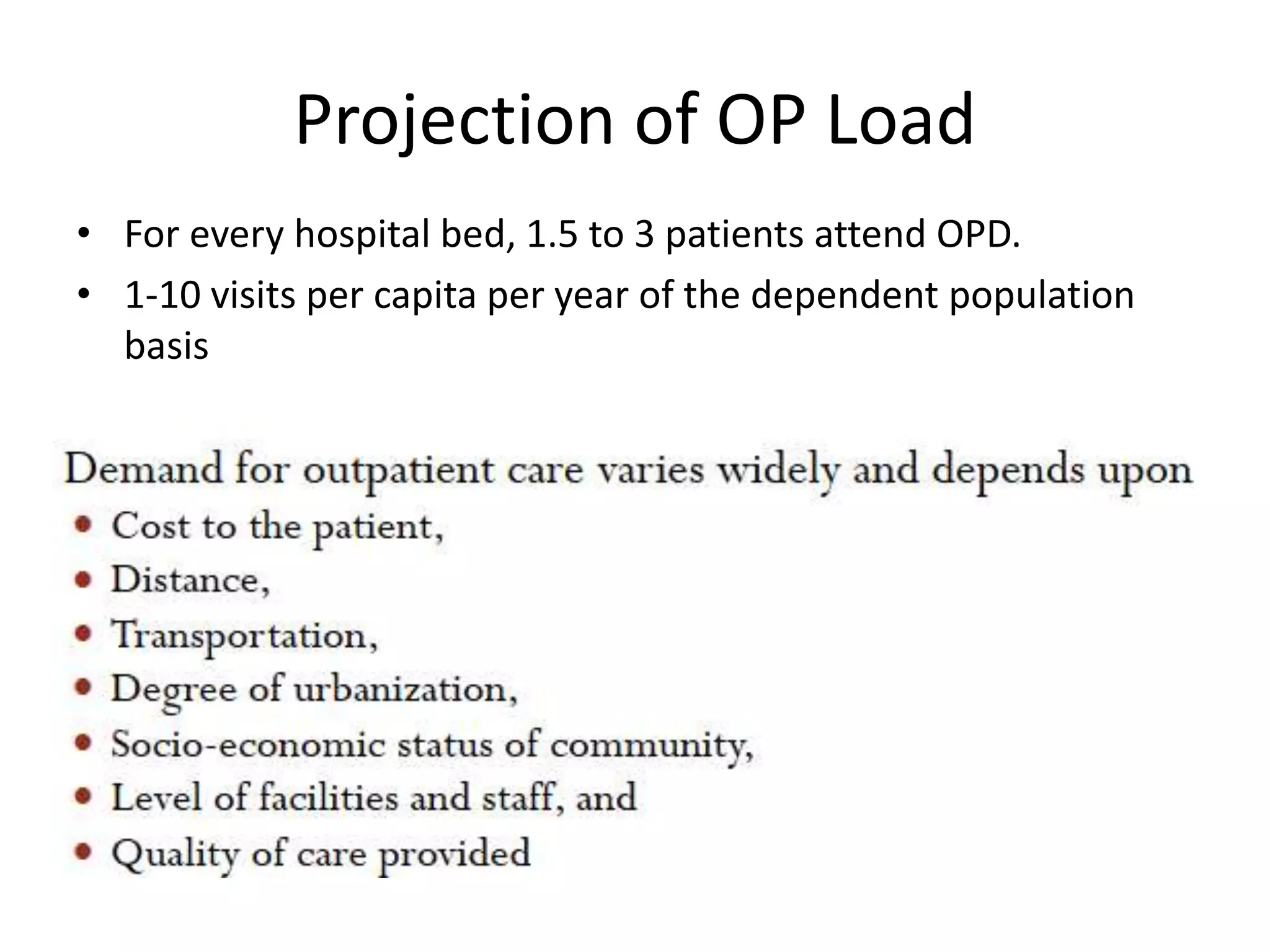
Shows statistics on patient services provided per bed, indicating the importance of OPD.
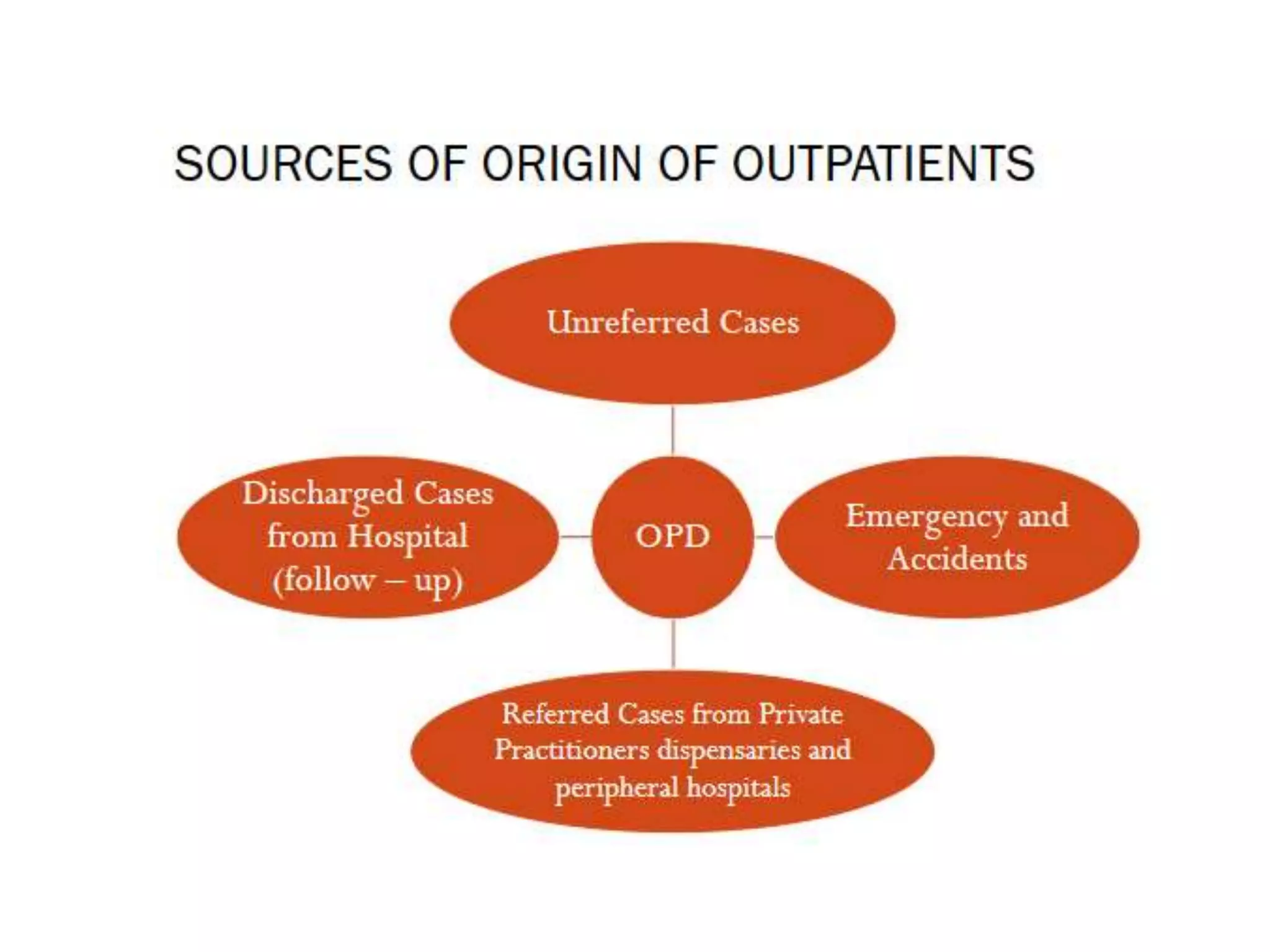
Lists various outpatient service types, including clinics, health centres, and their functions.
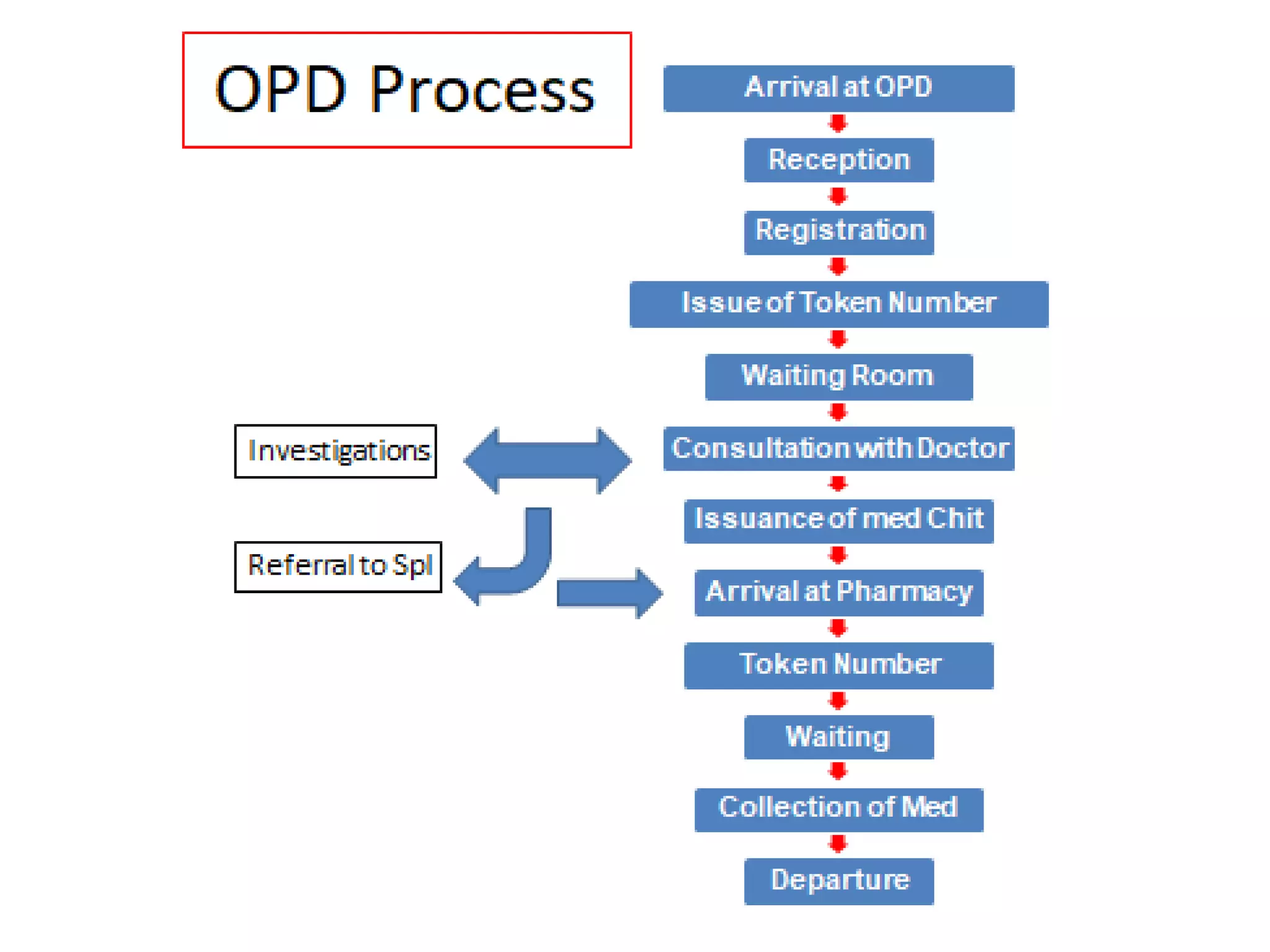
Discusses the links of OPD with hospitals and requirements for effective OPD service.
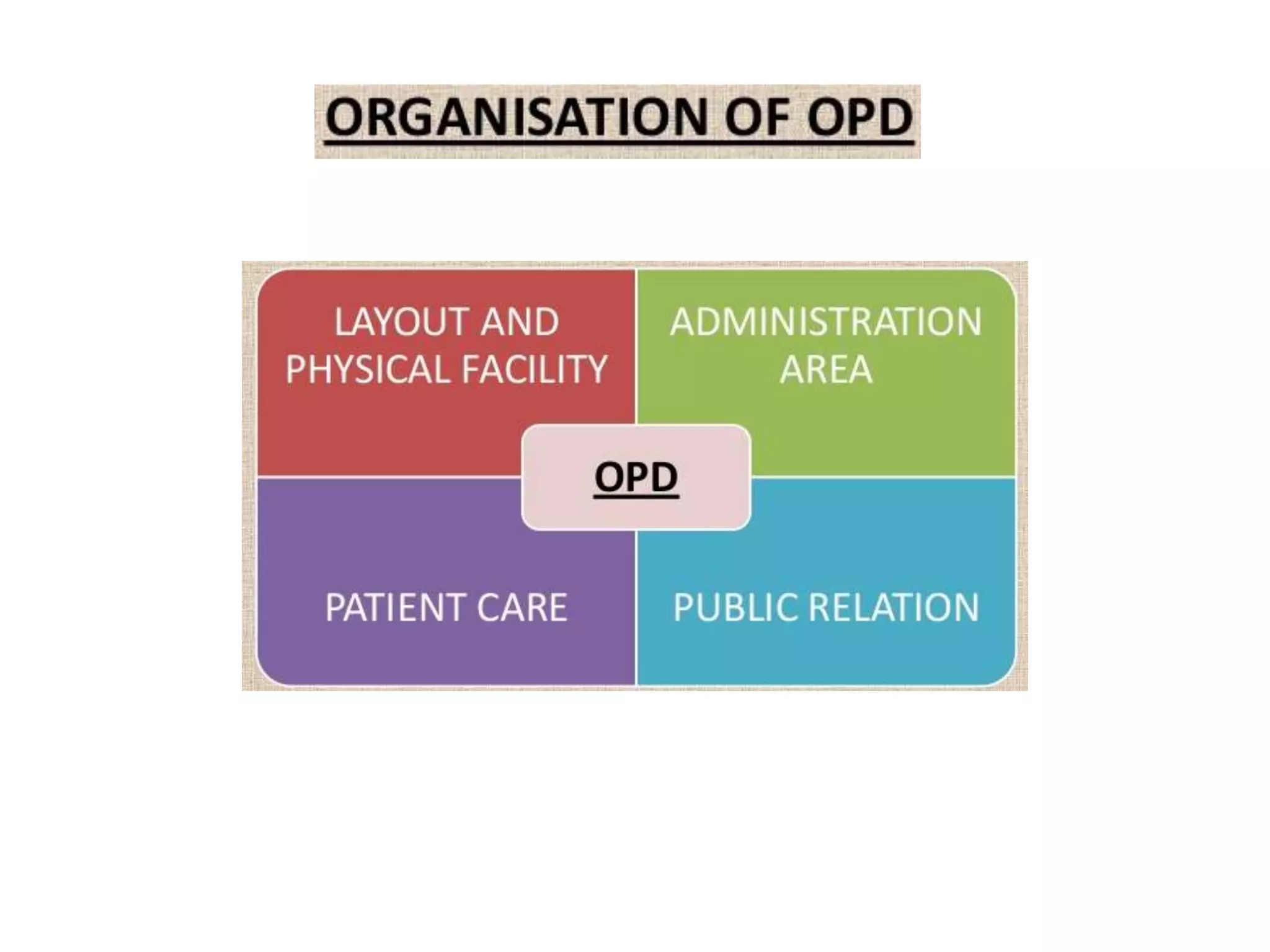
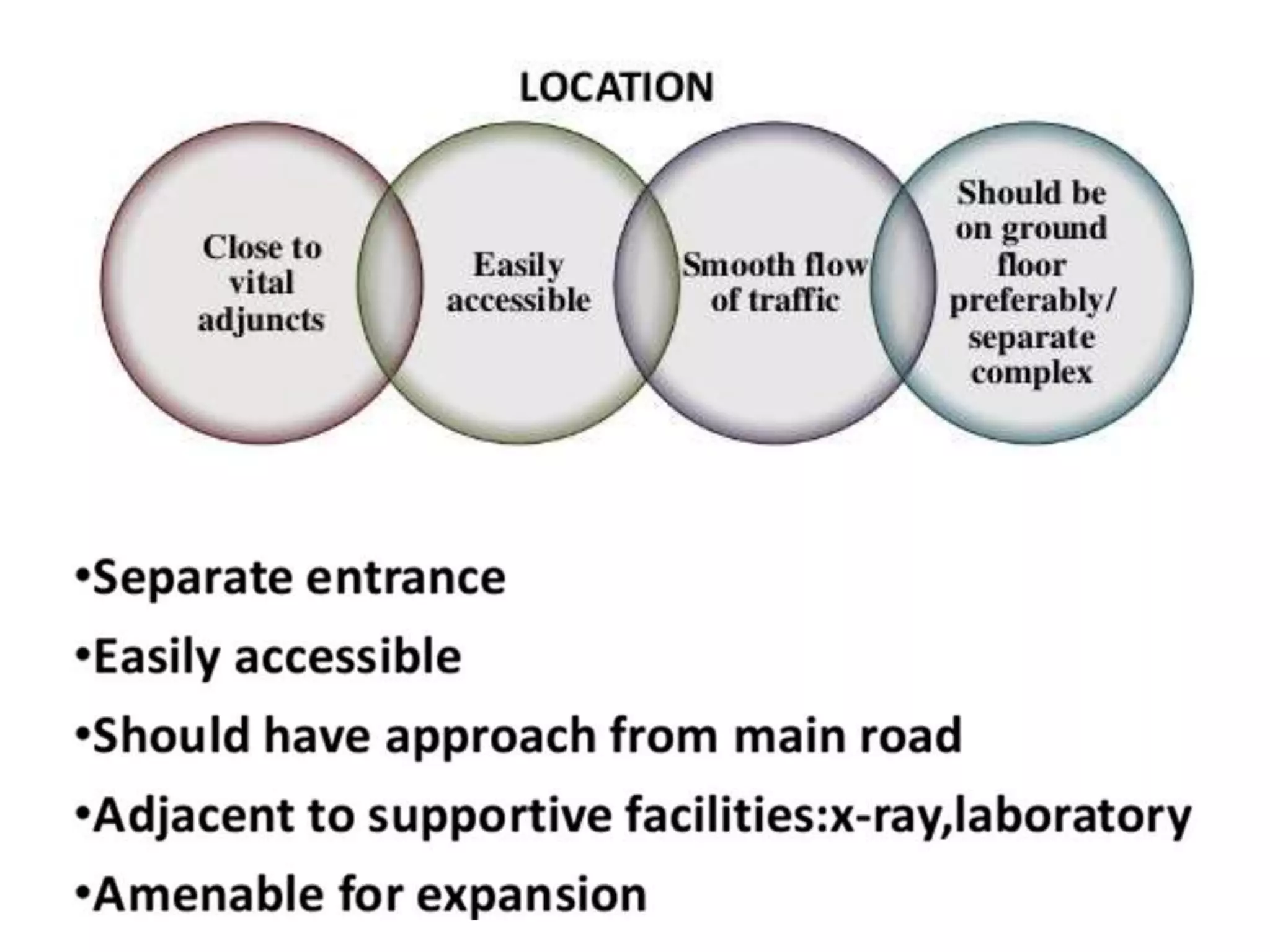
Focuses on design aspects and area requirements for efficient OPD functioning.
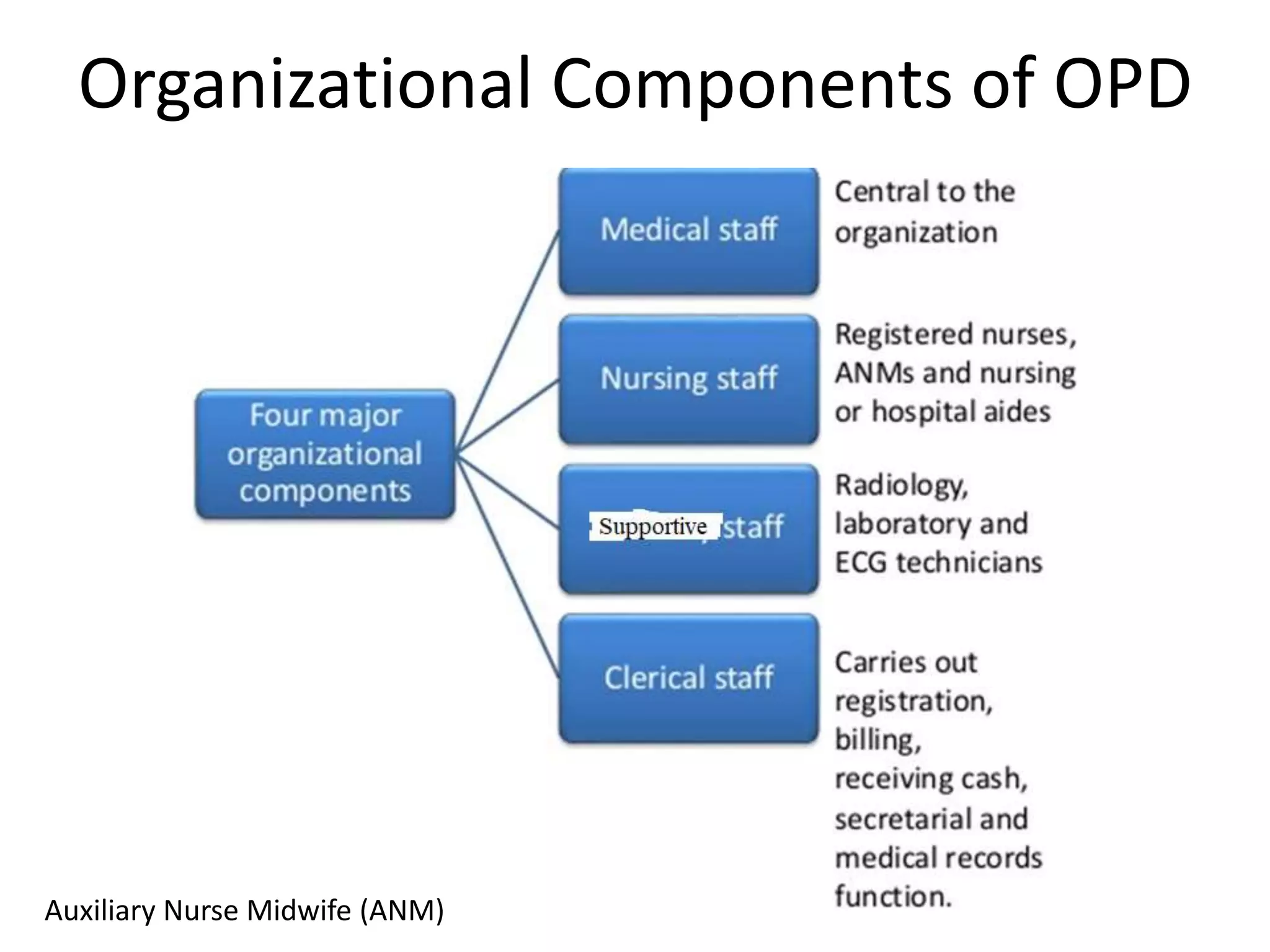
Details on administrative areas and circulation in OPD for operational efficiency.
Identifies general and specific problems within OPD including wait times and staffing issues.
Defines patient waiting time, benchmarks from the Institute of Medicine on acceptable wait durations.
Explains the reasons for long queues in OPDs, addressing capacity versus demand issues.
Provides solutions including appointment systems, patient education, and service design improvements.Discusses how perception of waiting time can affect patient satisfaction and queuing theory.
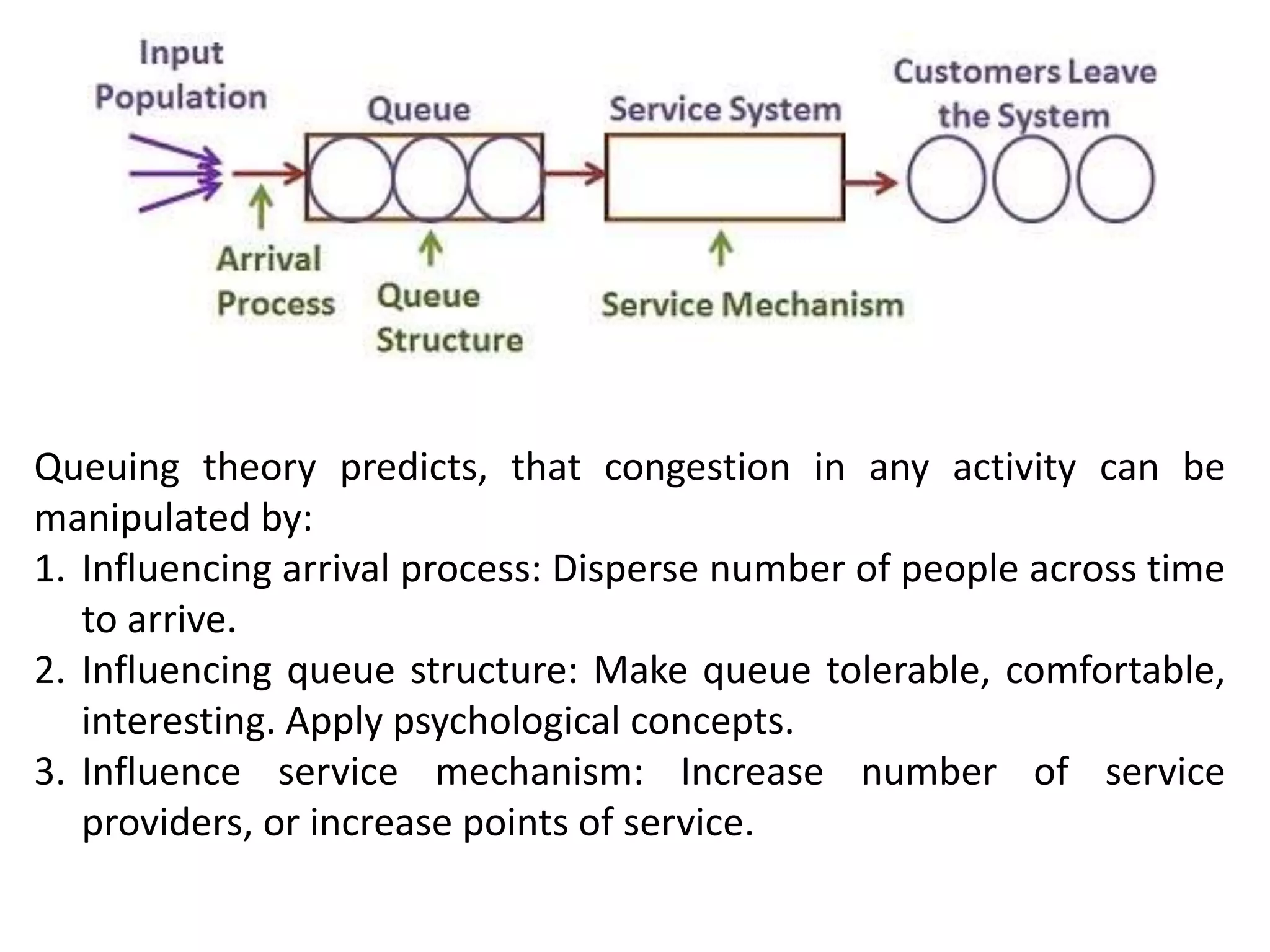
Describes methods to reduce waiting time through better system design and multiple queue management.
Suggestions for autoresponders and reminders in service optimization based on survey results.























































































