Download as PDF, PPTX

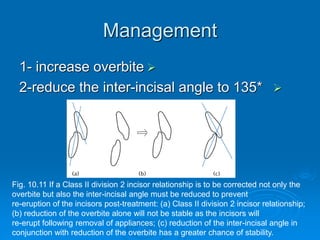
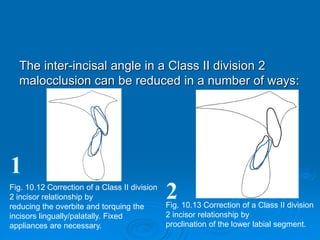
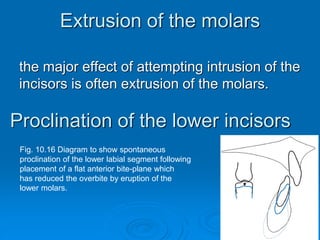
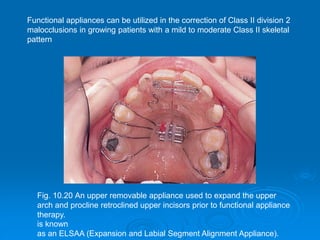

Class II division 2 malocclusions are characterized by retroclined upper central incisors with minimal overjet. They are commonly associated with a mild Class II skeletal pattern. The retroclined upper incisors can result from a high lower lip line relative to the upper incisors. Treatment aims to reduce the overbite and inter-incisal angle, such as by intruding the upper incisors with fixed appliances or proclining the lower incisors. Stable correction requires reducing both the overbite and inter-incisal angle to prevent relapse.