Download to read offline


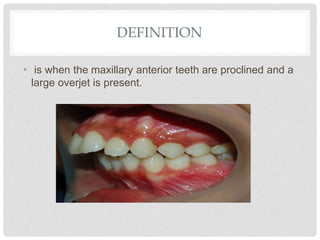
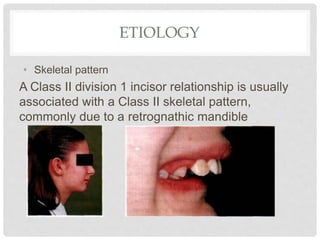
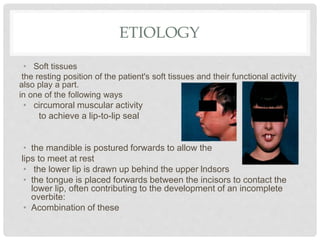

This document defines and discusses the etiology, features, assessment, treatment planning and management of Class II division 1 malocclusions. Key points include: - Class II division 1 malocclusions are characterized by proclined upper incisors and a large overjet. The etiology can include skeletal, dental, soft tissue and habit factors. - Treatment planning depends on factors like age, difficulty, stability, and facial aesthetics. It may involve early treatment, functional appliances, fixed appliances with/without extractions, or growth modification/orthodontic camouflage/surgery. - Stability after treatment requires full reduction of the overjet and achievement of lip competence through retention.





























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)





