
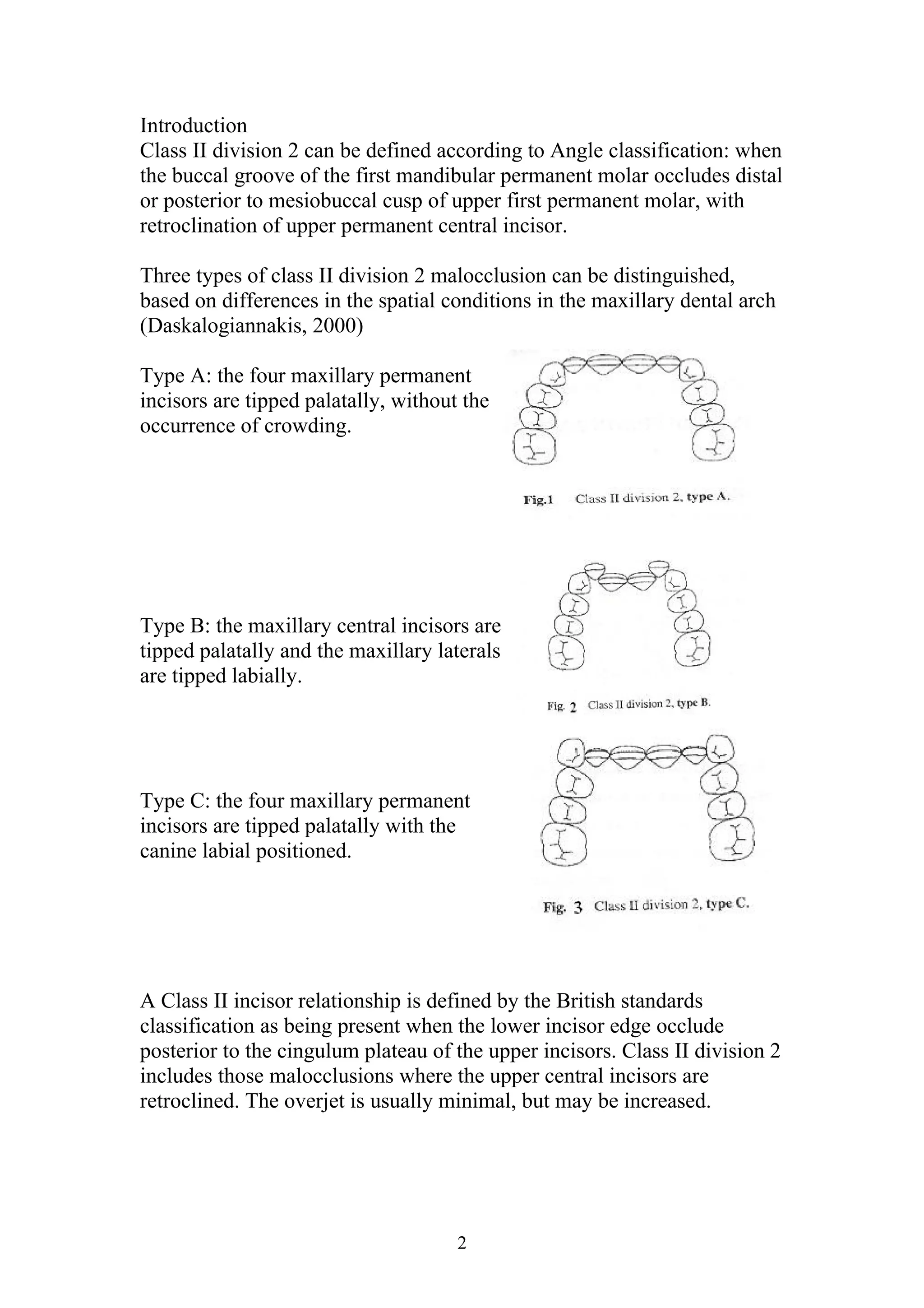

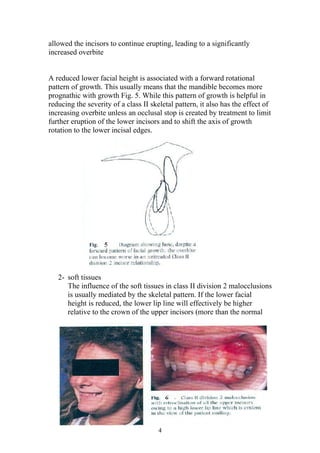
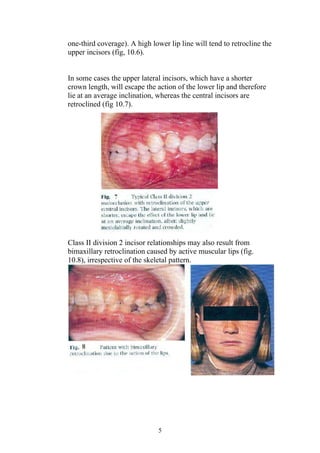

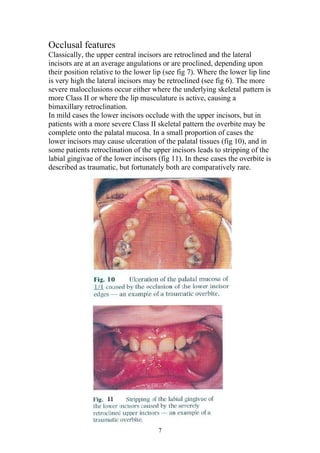






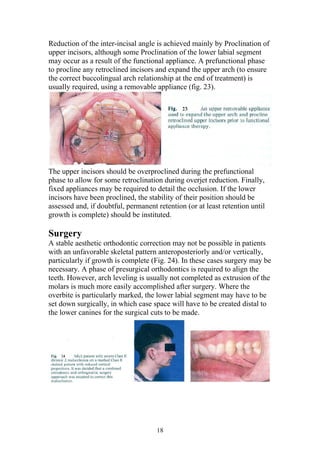





This document discusses Class II division 2 malocclusion. It defines the condition and describes three types (A, B, C) based on differences in the maxillary dental arch. The key features are a Class II relationship between the dental arches, retroclined upper incisors, and excessive overbite. Management options are to accept the incisor relationship if mild or correct it using various approaches like torquing incisor roots, proclining lower incisors, or a combination of methods. Treatment must reduce the inter-incisal angle and overbite to create an effective occlusal stop.









































































