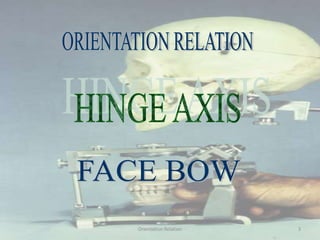
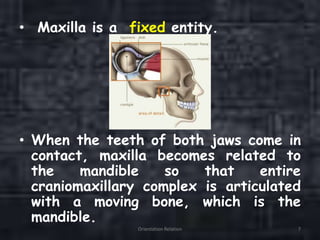
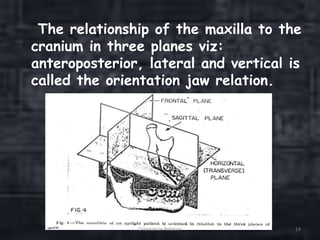
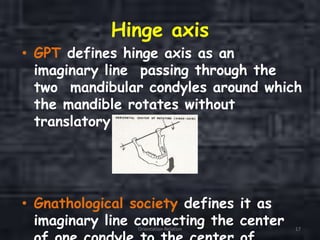
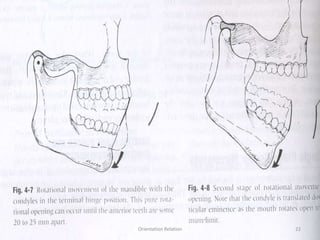
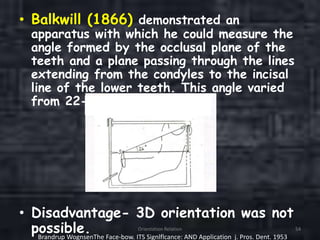
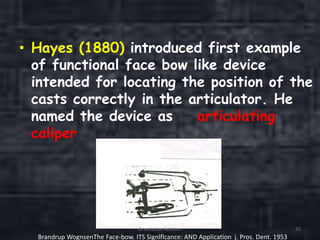
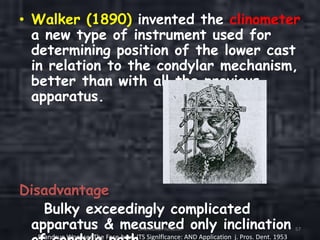
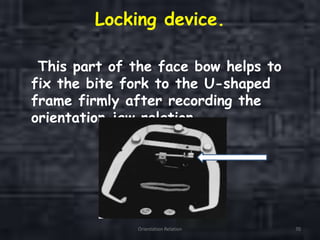
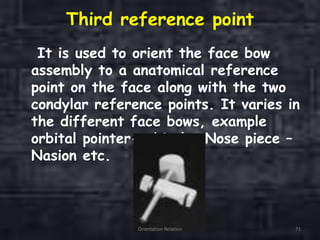
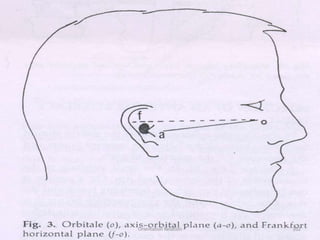
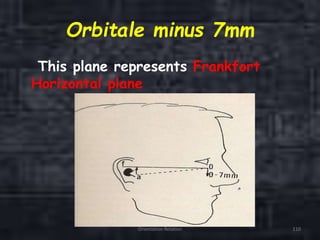
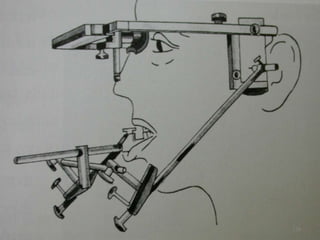
This document provides information about orientation jaw relations and the terminal hinge axis. It defines orientation jaw relations as the relationship between the maxilla and cranium in the anteroposterior, lateral, and vertical planes. It discusses how the terminal hinge axis is the axis around which pure rotation occurs when the mouth is opened widely and the condyles are in their most superior position. The document also reviews the history of debates around the hinge axis and different studies that have been conducted on the topic.










































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


