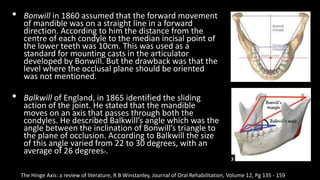
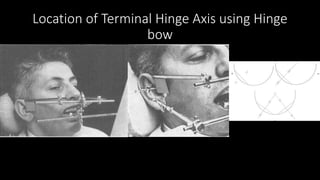
The document discusses the concept of the hinge axis, an imaginary line around which the mandible rotates within the sagittal plane, detailing its historical development, theories, and methods of localization. It outlines the types of mandibular movements (rotation and translation), reviews historical contributions from various figures in dentistry, and highlights the significance of the hinge axis in clinical practices. The document also presents different schools of thought regarding the location of the hinge axis and the advantages and disadvantages of various methods to locate it.