Downloaded 392 times


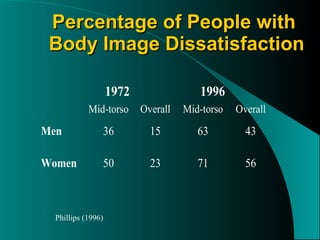

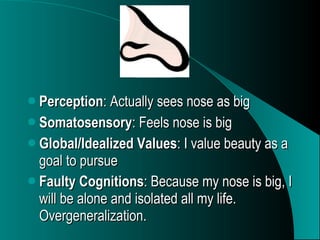





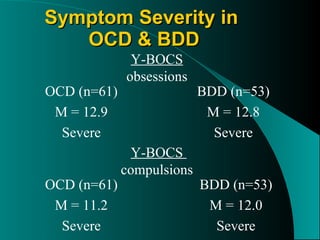
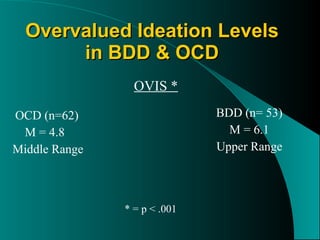
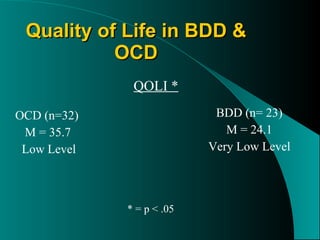
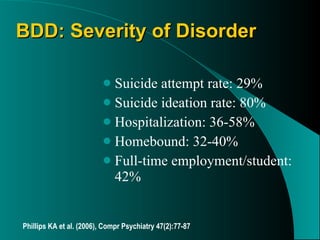



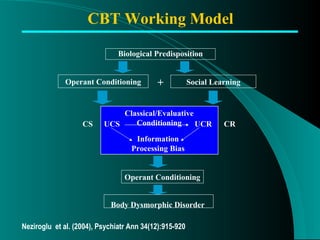
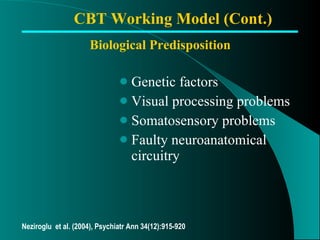

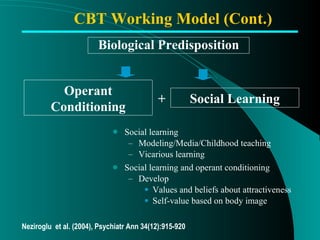
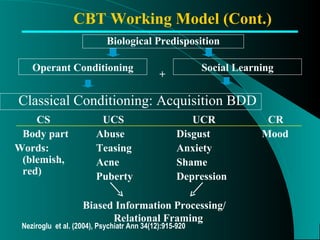

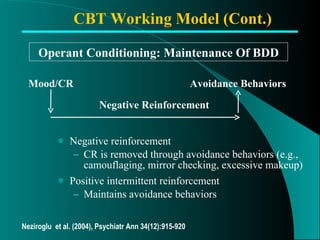
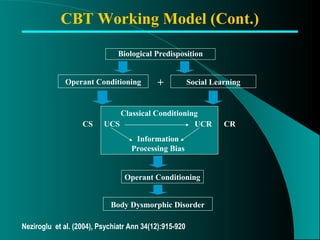


































The document discusses Body Dysmorphic Disorder (BDD) and Hypochondriasis. It compares the two disorders and outlines their key characteristics, including prevalence, demographics, comorbidities, and treatments. BDD involves a preoccupation with an imagined or slight defect in appearance. Hypochondriasis involves a preoccupation with fears of having a serious illness despite medical reassurance. Both disorders share similarities with OCD but also have distinct features and impacts on quality of life. Cognitive-behavioral therapy is an appropriate treatment approach for both.

















![Neurocognitive disorder [NCD]](https://cdn.slidesharecdn.com/ss_thumbnails/neurocognitivedisorderautosaved-201125072609-thumbnail.jpg?width=640&height=640&fit=bounds)





































































