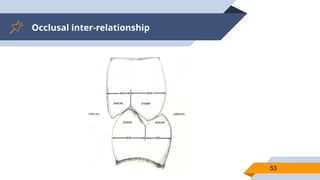
“Occlusion - Thestatic relationship between the
incising or masticating surfaces of the
maxillary and mandibular teeth. GPT -9
5
5
6.
“
Centric Relation [CR]- a maxillomandibular relationship,
independent of tooth contact, in which the condyles
articulate in the anterior-superior position against the
posterior slopes of the articular eminences; in this position,
the mandible is restricted to a purely rotary movement;
from this unstrained, physiologic, maxillomandibular
relationship, the patient can make vertical, lateral or
protrusive movements; it is a clinically useful, repeatable
reference position
GPT 9
6
6
7.
“
Centric Occlusion [CO]- the occlusion of opposing teeth
when the mandible is in centric relation; this may or may
not coincide with the maximal intercuspal position
Disclusion - the separation of opposing teeth during
eccentric movements of the mandible.
GPT 9
7
7
8.
“Maximum Intercuspation [MI]- It is the maximum
interdigitation of the maxillary teeth with the
mandibular teeth independent of condylar position.
GPT 9
8
8
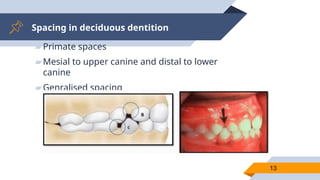
Spacing in deciduousdentition
▰Primate spaces
▰Mesial to upper canine and distal to lower
canine
▰Genralised spacing
13
14.
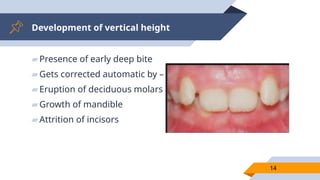
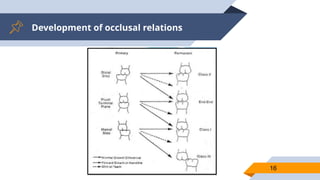
Development of verticalheight
▰Presence of early deep bite
▰Gets corrected automatic by –
▰Eruption of deciduous molars
▰Growth of mandible
▰Attrition of incisors
14
15.
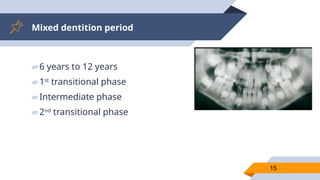
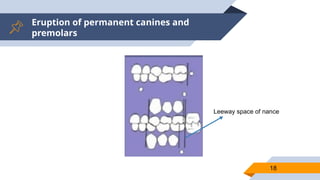
Mixed dentition period
▰6years to 12 years
▰1st
transitional phase
▰Intermediate phase
▰2nd
transitional phase
15
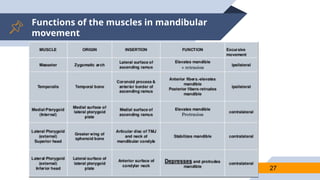
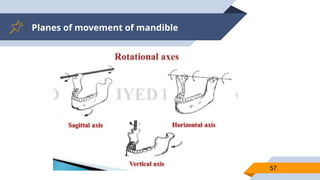
Posterior determinants ofocclusion
29
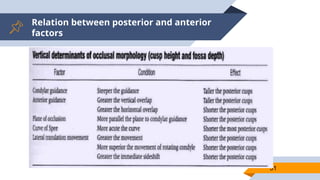
Stuart describes condylar factors as
determinants of occlusal morphology and
effect on acceptable cusp height and fossa
depth and allowable ridge and groove
direction of teeth, called as posterior
determinants of occlusion .
30.
Posterior determinants ofocclusion
30
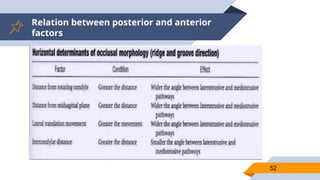
These are –
Path of the rotating condyle
Side shift
Path of orbiting condyle
Intercondylar distance
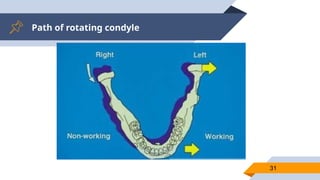
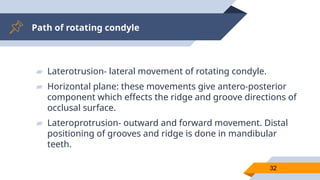
Path of rotatingcondyle
32
▰ Laterotrusion- lateral movement of rotating condyle.
▰ Horizontal plane: these movements give antero-posterior
component which effects the ridge and groove directions of
occlusal surface.
▰ Lateroprotrusion- outward and forward movement. Distal
positioning of grooves and ridge is done in mandibular
teeth.
33.
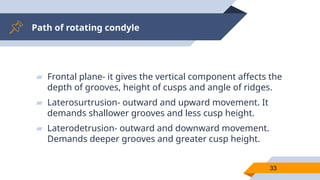
Path of rotatingcondyle
33
▰ Frontal plane- it gives the vertical component affects the
depth of grooves, height of cusps and angle of ridges.
▰ Laterosurtrusion- outward and upward movement. It
demands shallower grooves and less cusp height.
▰ Laterodetrusion- outward and downward movement.
Demands deeper grooves and greater cusp height.
34.
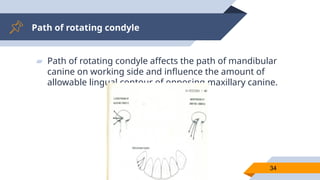
Path of rotatingcondyle
34
▰ Path of rotating condyle affects the path of mandibular
canine on working side and influence the amount of
allowable lingual contour of opposing maxillary canine.
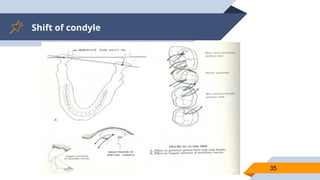
Shift of condyle
36
lateralshifting of mandible as lateral movement is made. This is
produced by combination of rotation and translation in both
horizontal and frontal planes.
Greater the immediate shift, shorter is allowable cusp height.
If Presence immediate shift also requires mesial positioning of
grooves and ridges of mandibular teeth and more distal
positioning of oblique ridges and grooves of maxillary teeth.
During right lateral movement, greater mediotrusion of left
condyle that is produced by side shift, greater must lingual
concavity of maxillary canine in order to allow smooth cyclic
chewing movement without conflict.
37.
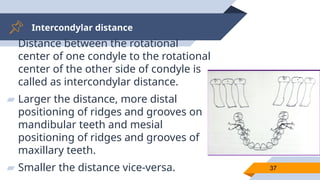
Intercondylar distance
37
▰ Distancebetween the rotational
center of one condyle to the rotational
center of the other side of condyle is
called as intercondylar distance.
▰ Larger the distance, more distal
positioning of ridges and grooves on
mandibular teeth and mesial
positioning of ridges and grooves of
maxillary teeth.
▰ Smaller the distance vice-versa.
38.
Path of orbitingcondyle
38
This is the detrusion of orbiting(non working)
condyle in relation to horizontal cranial reference
plane.
Greater angle of the path, greater cusp height
and deeper the fossa.
Anterior determinants ofocclusion
40
▰ The factors within dentition which influences the
mandibular movement are called as anterior determinants of
occlusion.
▰ These are –
▰ Occlusal plane
▰ Compensating curves
▰ Vertical and horizontal overlap of anterior teeth
41.
Occlusal plane
41
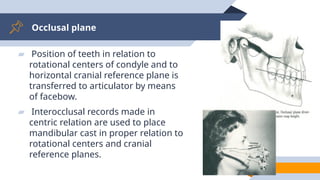
▰ Positionof teeth in relation to
rotational centers of condyle and to
horizontal cranial reference plane is
transferred to articulator by means
of facebow.
▰ Interocclusal records made in
centric relation are used to place
mandibular cast in proper relation to
rotational centers and cranial
reference planes.
Compensating curves
43
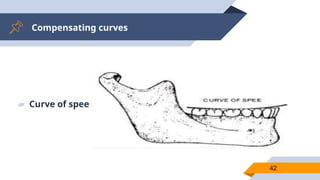
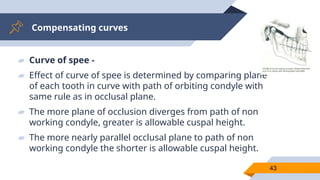
▰ Curveof spee -
▰ Effect of curve of spee is determined by comparing plane
of each tooth in curve with path of orbiting condyle with
same rule as in occlusal plane.
▰ The more plane of occlusion diverges from path of non
working condyle, greater is allowable cuspal height.
▰ The more nearly parallel occlusal plane to path of non
working condyle the shorter is allowable cuspal height.
44.
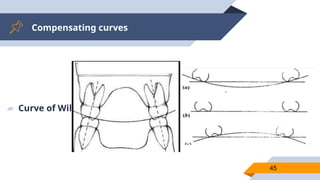
Compensating curves
44
▰ Curveof Willson -
▰ ■ It is an imaginary lateral curve.
▰ ■ Its convexity faces upwards in 1st premolars.
▰ ■ It become straight in 2nd premolars
▰ ■ And faces downwards in molars.
▰ ■ In complete denture occlusion it is called lateral
compensating curve
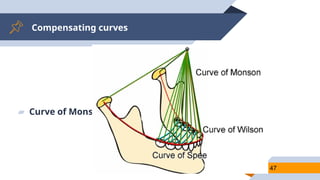
Compensating curves
46
▰ Curveof Monson –
▰ Extending the curve of Spee and Willson to all cusps and
incisal edges reveals the curve of Monson. Combination of
curve of spee and willson, 3D curve.
Vertical and horizontaloverlap of
anterior teeth
49
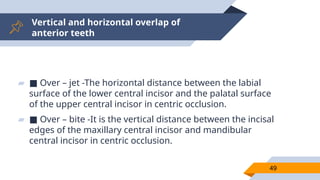
▰ ■ Over – jet -The horizontal distance between the labial
surface of the lower central incisor and the palatal surface
of the upper central incisor in centric occlusion.
▰ ■ Over – bite -It is the vertical distance between the incisal
edges of the maxillary central incisor and mandibular
central incisor in centric occlusion.
50.
Vertical and horizontaloverlap of
anterior teeth
50
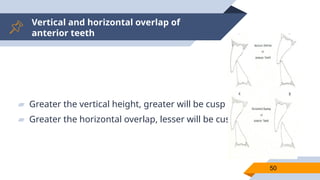
▰ Greater the vertical height, greater will be cusp height.
▰ Greater the horizontal overlap, lesser will be cusp height.
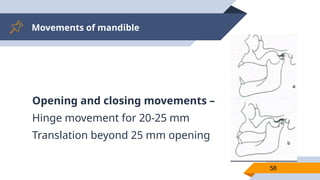
Movements of mandible
59
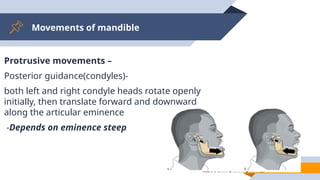
Protrusivemovements –
Posterior guidance(condyles)-
both left and right condyle heads rotate openly
initially, then translate forward and downward
along the articular eminence
-Depends on eminence steep
60.
Movements of mandible
60
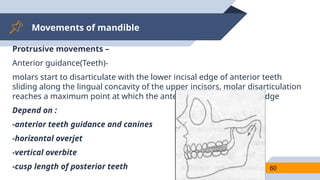
Protrusivemovements –
Anterior guidance(Teeth)-
molars start to disarticulate with the lower incisal edge of anterior teeth
sliding along the lingual concavity of the upper incisors, molar disarticulation
reaches a maximum point at which the anterior teeth are edge-to-edge
Depend on :
-anterior teeth guidance and canines
-horizontal overjet
-vertical overbite
-cusp length of posterior teeth
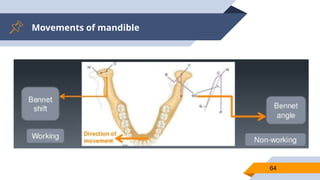
Movements of mandible
62
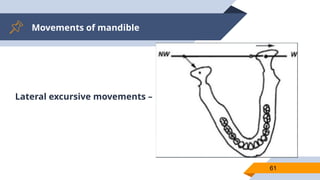
Lateralexcursive movements –
Posterior guidance (condyles):
The condyle at the side which the mandible is moving towards is called
the working condyle , it rotates forward and translates slightly lateral
The slight lateral movement is immediate, non progressive and
described as ‘immediate side shift’, or ‘Bennet movement’.
Its described in 86% of lateral movement and is about 0.5 to 3 mm
63.
Movements of mandible
63
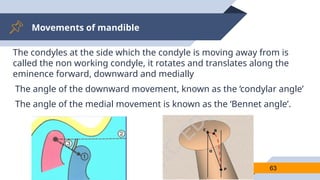
Thecondyles at the side which the condyle is moving away from is
called the non working condyle, it rotates and translates along the
eminence forward, downward and medially
The angle of the downward movement, known as the ‘condylar angle’
The angle of the medial movement is known as the ‘Bennet angle’.
Movements of mandible
65
Anteriorguidance(teeth)–
Canine guidance :
the sliding action contact between cusps of the opposing canines on
the working side disarticulate the teeth on the non-working side
If any other premature contact between any other teeth happens on
working and/or non-working side , is an interference
66.
Movements of mandible
66
Anteriorguidance(teeth)–
Or Group function :
The sliding contact between cusps of the opposing canines,
premolars, and molars on the working side; disarticulate all teeth on
the non-working side
If any other contact on the non-working side only happens is an
interference
Mutually protected occlusion
68
Anocclusal scheme in which the posterior teeth prevent excessive
contact of the anterior teeth in maximum intercuspation, and the
anterior teeth disengage the posterior teeth in all mandibular
excursive movements.
Advantages
70
1) 1) Minimumamount of tooth contact is involved and this makes
for better penetration of the food.
2) 2) The force is closer to the long axis of each tooth.
3) 3) The arrangement of the marginal, transverse and oblique ridges
so that they have a shearing action, which makes for a much more
chewing apparatus.
4) 4) better health of teeth not in function.
71.
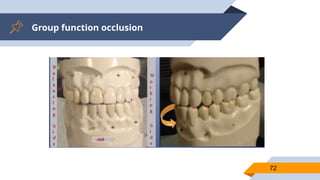
Group function occlusion
71
Multiplecontact relations between the maxillary and mandibular teeth
in lateral movements on the working side whereby simultaneous
contact of several teeth acts as a group to distribute occlusal forces.
Advantages
73
1) Lateral pressureare distributed to all working side tooth.
2) Long centric, so allow some freedom of movement in an
anteroposterior direction.
74.
Balanced occlusion
74
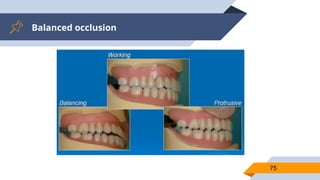
1) Thebilateral, simultaneous, anterior, and posterior occlusal
contact of teeth in centric and eccentric positions.
Advantages
76
1) 1) Helpto seat the denture in a stable position during function.
2) 2) Patients do not upset the normal static, stable, and retentive
position of their dentures.
3) 3) In balanced occlusion, the denture bases are stable during
bruxing activity.
77.
Occlusion in naturaldentition
77
1) • Posterior disclusion on protrusion
2) • Disclusion on non working side during lateral movement.
3) • Occlusion on working side (either canine guided/group function)
during lateral movement.
78.
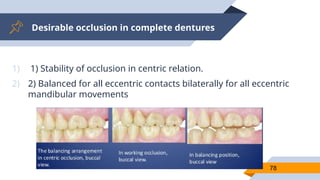
Desirable occlusion incomplete dentures
78
1) 1) Stability of occlusion in centric relation.
2) 2) Balanced for all eccentric contacts bilaterally for all eccentric
mandibular movements
79.
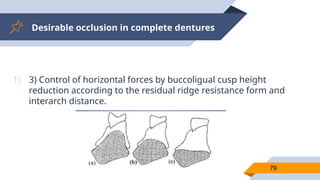
Desirable occlusion incomplete dentures
79
1) 3) Control of horizontal forces by buccoligual cusp height
reduction according to the residual ridge resistance form and
interarch distance.
80.
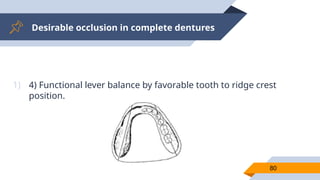
Desirable occlusion incomplete dentures
80
1) 4) Functional lever balance by favorable tooth to ridge crest
position.
81.
Desirable occlusion incomplete dentures
81
1) 5) Unlocking the cusp mesiodistally to allow for gradual but
inevitable settling of the bases due to tissue deformation and
bone resorption.
2) 6) Cutting and shearing efficiency of the occlusal surface (sharp
cusps or ridges).
3) 7) Anterior clearance of teeth during mastication. Minimum
occlusal contact between the upper and lower teeth to reduce
pressure during function.
82.
Desirable occlusion inRemovable partial
dentures
82
1) Kennedy’s class 1 situation –
2) Mandibular RPD vs natural dentition
3) Working side- contact
4) Balancing side no contact
83.
Desirable occlusion inRemovable partial
dentures
83
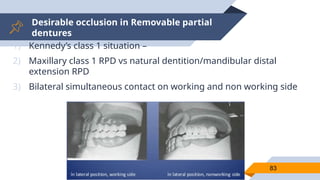
1) Kennedy’s class 1 situation –
2) Maxillary class 1 RPD vs natural dentition/mandibular distal
extension RPD
3) Bilateral simultaneous contact on working and non working side
84.
Desirable occlusion inRemovable partial
dentures
84
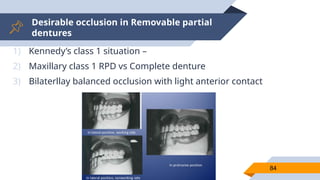
1) Kennedy’s class 1 situation –
2) Maxillary class 1 RPD vs Complete denture
3) Bilaterllay balanced occlusion with light anterior contact
85.
Desirable occlusion inRemovable partial
dentures
85
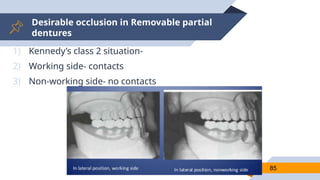
1) Kennedy’s class 2 situation-
2) Working side- contacts
3) Non-working side- no contacts
86.
Desirable occlusion inRemovable partial
dentures
86
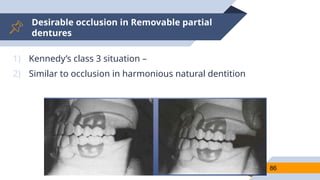
1) Kennedy’s class 3 situation –
2) Similar to occlusion in harmonious natural dentition
87.
Desirable occlusion inRemovable partial
dentures
87
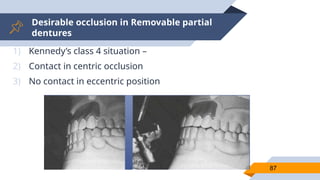
1) Kennedy’s class 4 situation –
2) Contact in centric occlusion
3) No contact in eccentric position
88.
Desirable occlusion inFixed partial
dentures
88
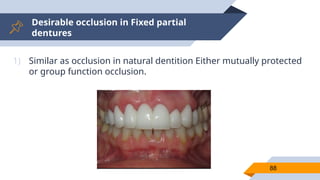
1) Similar as occlusion in natural dentition Either mutually protected
or group function occlusion.
89.
Desirable occlusion inFixed partial
dentures
89
1) In the following cases, desirable occlusion should be group
function –
2) Periodontally compromised supporting anterior teeth.
3) Missing canine
4) Angle class-II and class-III malocclusion
5) Crossbite
90.
Desirable occlusion inosseointegrated
prosthesis
90
1) 1) Full-arch fixed prosthesis –
2) Bilateral balanced occlusion with opposing complete denture
3) Group function occlusion or
4) mutually protected occlusion with shallow anterior guidance when
opposing natural dentition Freedom in centric (1–1.5mm)
5) 2) Overdenture –
6) Bilateral balanced occlusion using lingualized occlusion
7) Monoplane occlusion on a severely resorbed ridge




![“
Centric Relation [CR] - a maxillomandibular relationship,
independent of tooth contact, in which the condyles
articulate in the anterior-superior position against the
posterior slopes of the articular eminences; in this position,
the mandible is restricted to a purely rotary movement;
from this unstrained, physiologic, maxillomandibular
relationship, the patient can make vertical, lateral or
protrusive movements; it is a clinically useful, repeatable
reference position
GPT 9
6
6](https://image.slidesharecdn.com/occlusioninprosthodontics-250811152041-237a540a/85/occlusion-in-prosthodontic-dentistry-ppt-6-320.jpg)
![“
Centric Occlusion [CO] - the occlusion of opposing teeth
when the mandible is in centric relation; this may or may
not coincide with the maximal intercuspal position
Disclusion - the separation of opposing teeth during
eccentric movements of the mandible.
GPT 9
7
7](https://image.slidesharecdn.com/occlusioninprosthodontics-250811152041-237a540a/85/occlusion-in-prosthodontic-dentistry-ppt-7-320.jpg)
![“Maximum Intercuspation [MI] - It is the maximum
interdigitation of the maxillary teeth with the
mandibular teeth independent of condylar position.
GPT 9
8
8](https://image.slidesharecdn.com/occlusioninprosthodontics-250811152041-237a540a/85/occlusion-in-prosthodontic-dentistry-ppt-8-320.jpg)























![occlusion mmmmmmmm- Copy [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/occlusion-copyautosaved-240715160312-7fd34768-thumbnail.jpg?width=640&height=640&fit=bounds)

















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)





