Downloaded 65 times
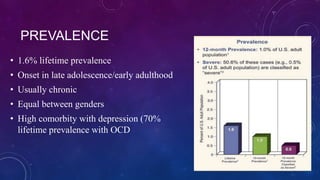



This document provides information about obsessive-compulsive disorder (OCD). It discusses the prevalence of OCD, noting it has a lifetime prevalence of 1.6% and typically has an onset in late adolescence/early adulthood. It is usually chronic and equally affects both genders. The document also examines the pathology of OCD, including increased activity in brain regions like the basal ganglia, orbitofrontal cortex, and thalamus. Signs and symptoms include obsessions, compulsions, and repetitive behaviors. Treatments discussed are cognitive behavioral therapy, pharmacotherapy using SSRIs, and psychosurgery for severe cases.




![Neurocognitive Disorders [2020]](https://cdn.slidesharecdn.com/ss_thumbnails/ncd2020v2-200526001756-thumbnail.jpg?width=640&height=640&fit=bounds)