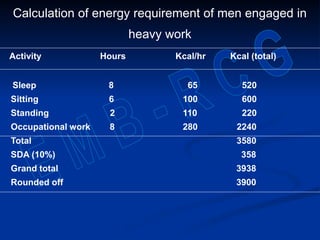
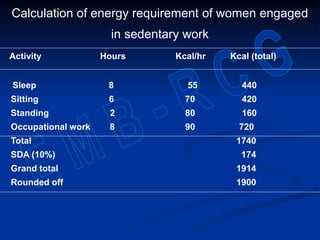
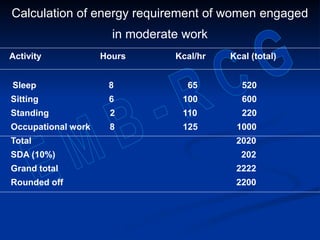
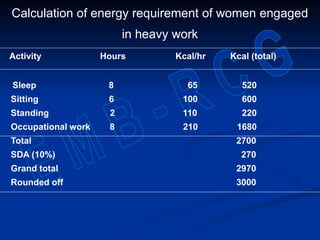
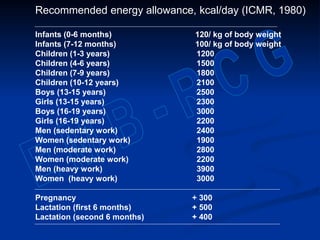
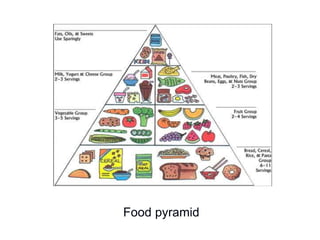
This document discusses nutrition, diet, and energy requirements. It defines key units of energy like calories and explains how the caloric values of macronutrients are measured. Carbohydrates have 4 calories per gram, lipids have 9 calories per gram, and proteins have 4 calories per gram. Energy expenditure is influenced by factors like basal metabolic rate, specific dynamic action of food, and physical activity levels. The document provides calculations to determine recommended daily energy intake for Indian men and women based on their activity levels.


















![ A simpler alternative is the calculation of body
mass index (BMI)
BMI =
The normal BMI is 20 -25 in males and 19 - 24
in females
A BMI above the upper limit of normal signifies
obesity
Weight in kg
[Height in metres]2](https://image.slidesharecdn.com/nutritionanddiet-231118072636-ce3411e4/85/Nutrition-and-Diet-ppt-183-320.jpg)