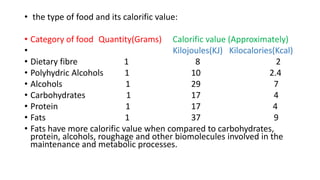
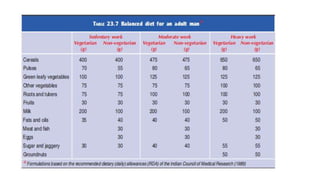
Calories and calorific values are units used to measure the energy content of foods. A calorie is the amount of heat needed to raise 1 gram of water by 1°C, while a kilocalorie (kcal) is equal to 1000 calories. Fats have the highest calorific value at 9 kcal/gram, while proteins and carbohydrates are both 4 kcal/gram. Basal metabolic rate (BMR) is the minimum energy needed to sustain life at rest, and varies based on factors like surface area, sex, age, and disease states. Specific dynamic action refers to the extra calories expended when digesting and metabolizing foods. A balanced diet provides adequate nutrients from different food












































![Medical Biochemistry Card 2 Item 1 [part 2]](https://cdn.slidesharecdn.com/ss_thumbnails/foodnutritionfinaltoday-200422145412-thumbnail.jpg?width=640&height=640&fit=bounds)

























