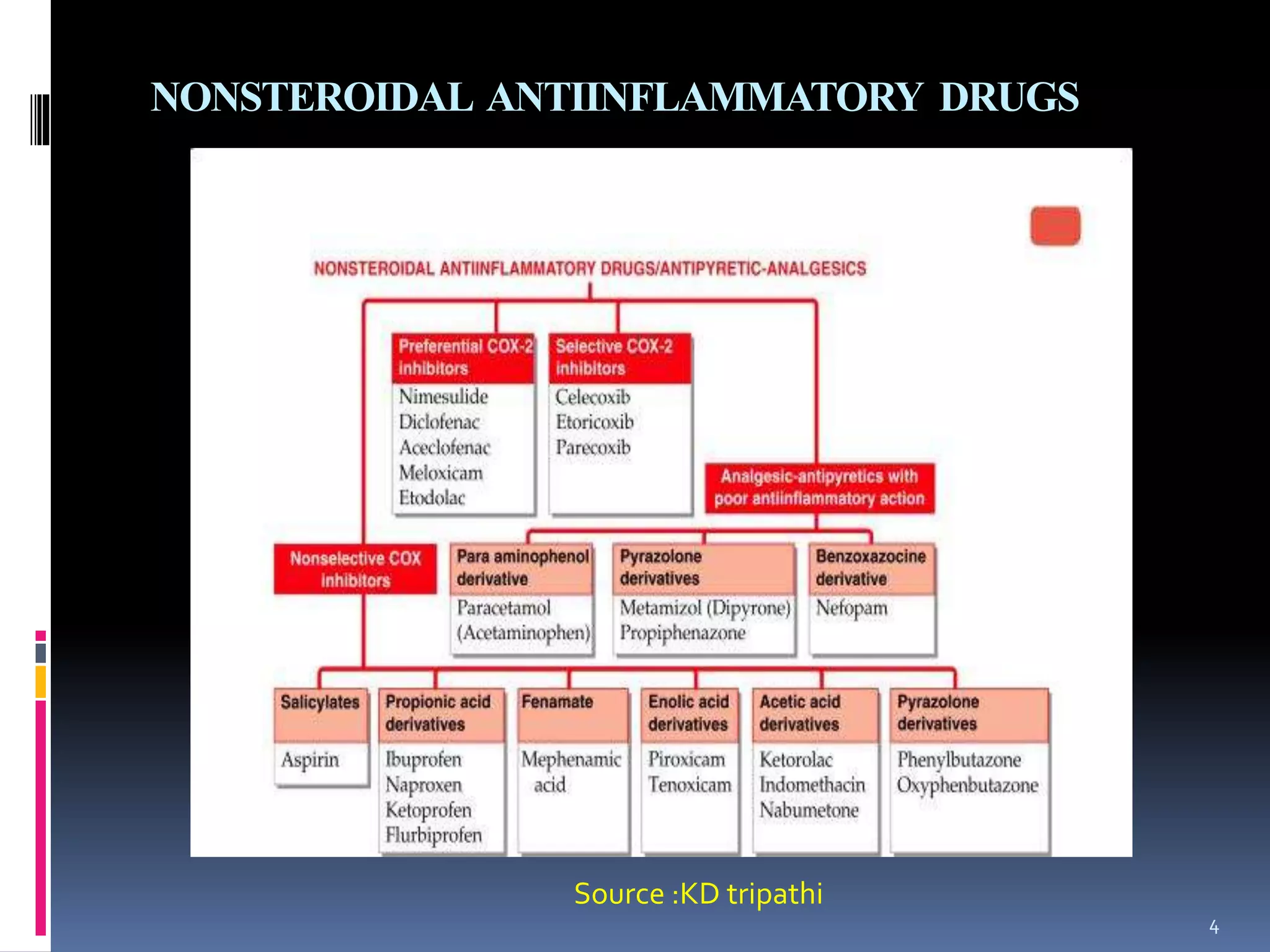
This document provides an overview of non-narcotic analgesics, also known as nonsteroidal anti-inflammatory drugs (NSAIDs). It discusses the mechanisms of action and pharmacological properties of various classes of NSAIDs, including salicylates, para-aminophenol derivatives, propionic acid derivatives, acetic acid derivatives, pyrazolone derivatives, and oxicam derivatives. The document also covers preferential and selective COX-2 inhibitors as well as factors to consider when choosing an appropriate NSAID for different pain conditions.