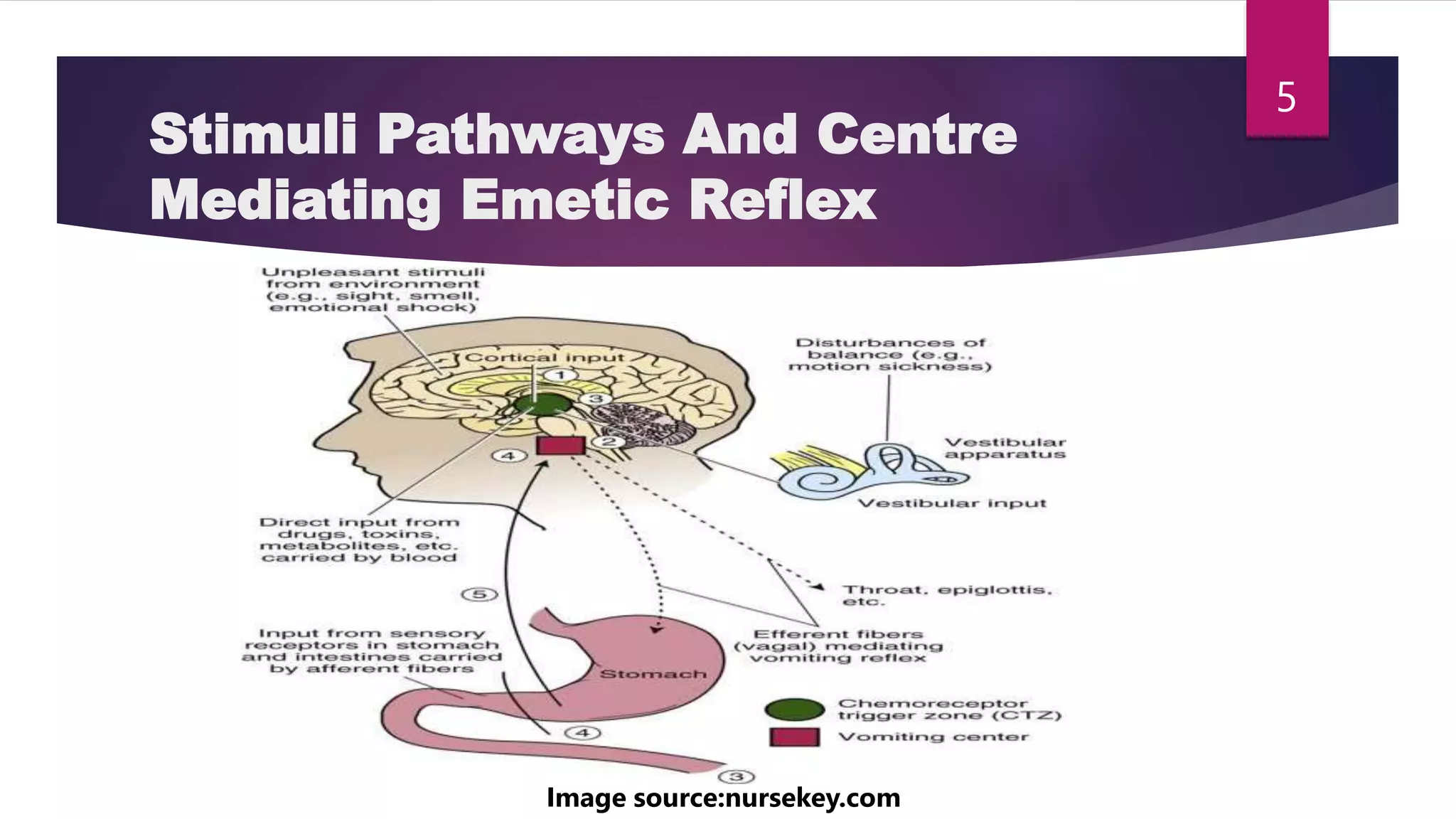
This document discusses antiemetics and prokinetics. It begins by describing the physiology of vomiting and stimuli pathways and centers that mediate the emetic reflex. It then covers various classes of antiemetics including dopamine D2 antagonists, 5-HT3 antagonists, antimuscarinics, neuroleptics, and other agents. Prokinetics are also discussed, focusing on their mechanisms of action to enhance gastrointestinal motility. Common prokinetic drugs like metoclopramide, cisapride, and erythromycin are described along with their uses and adverse effects.