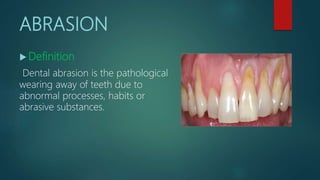
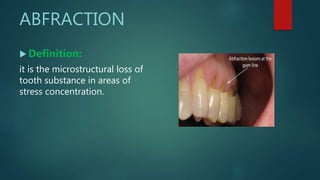
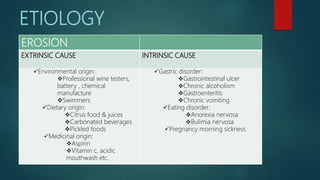
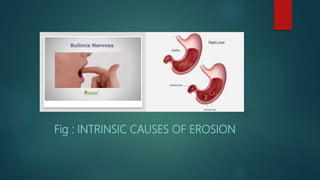
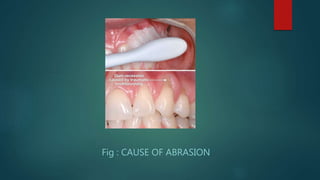
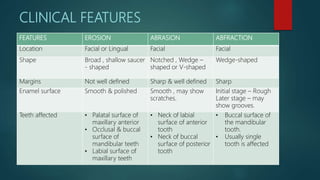
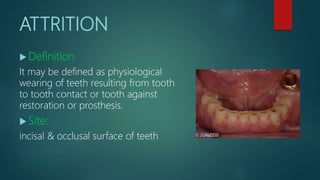
This document discusses non-carious tooth surface loss including erosion, abrasion, abfraction, and attrition. It defines each type of lesion, describes their causes, clinical features, diagnosis, and treatment options. Erosion is caused by chemical dissolution from acids, while abrasion results from mechanical forces from toothbrushing or habits. Abfraction is microstructural loss from occlusal stresses. Attrition is normal wear from tooth contact. Prevention focuses on diet, oral habits, and correcting occlusal issues. Treatment includes restoration, endodontics, and protecting teeth from further loss.