Downloaded 507 times


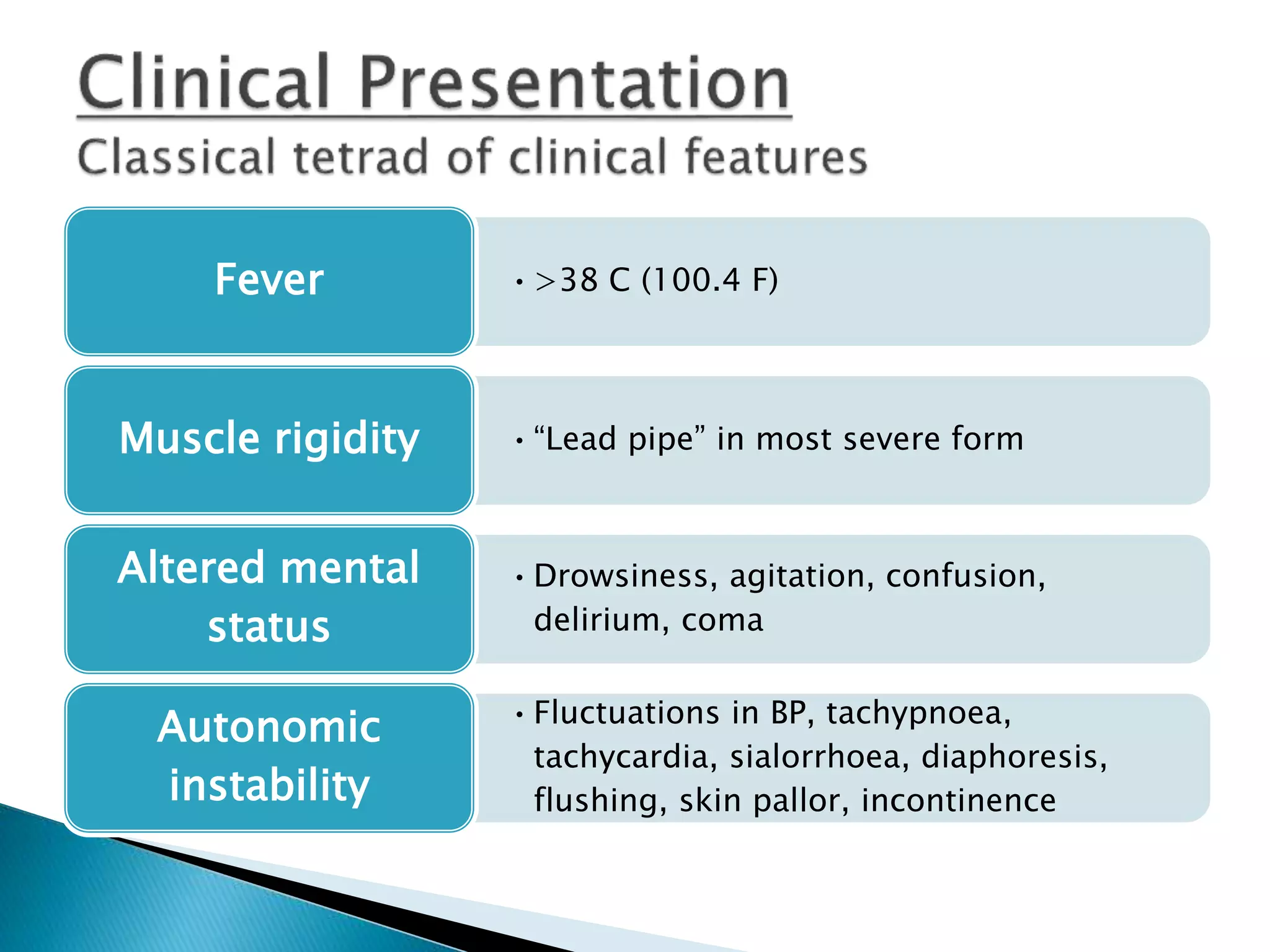
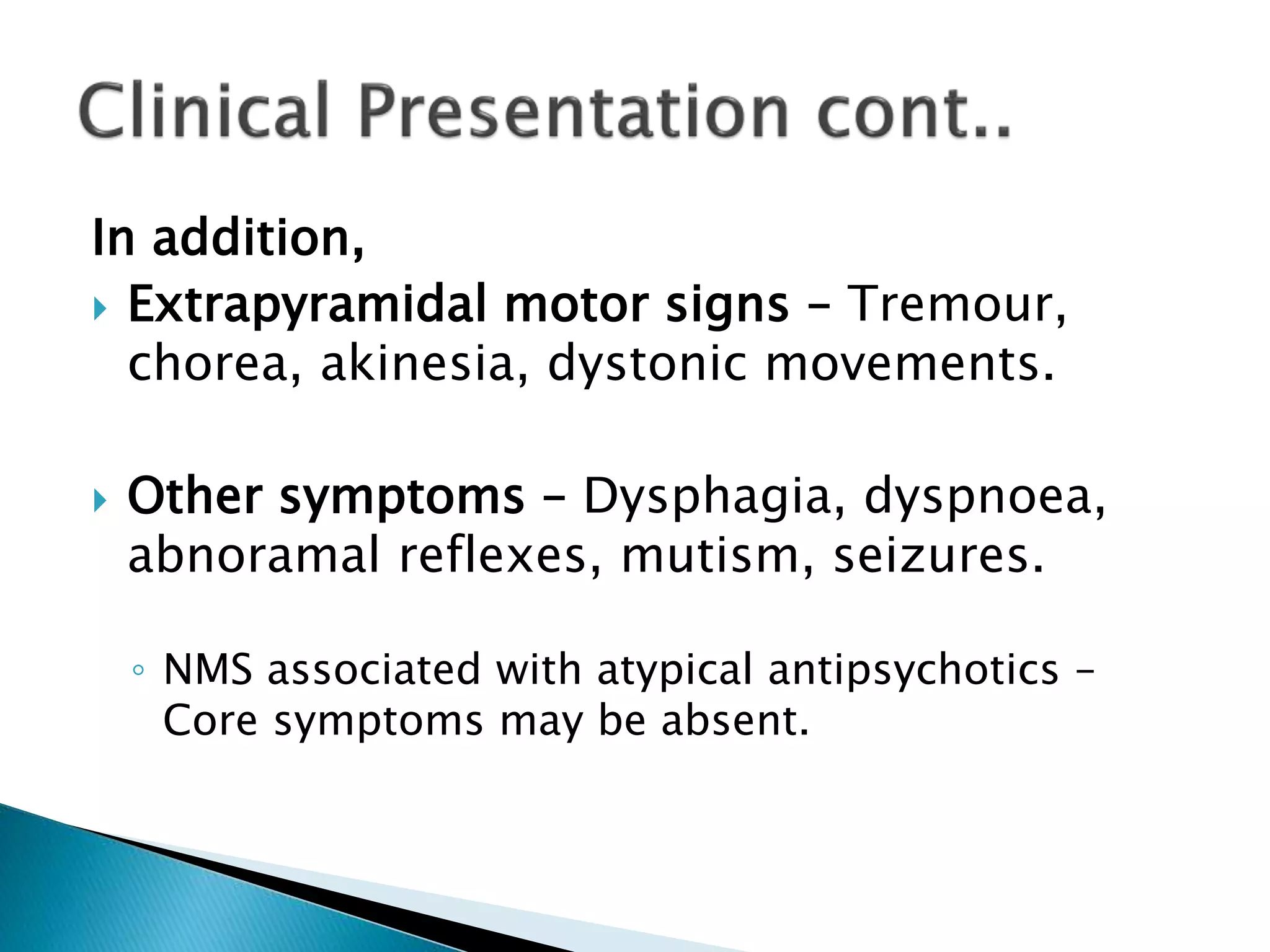



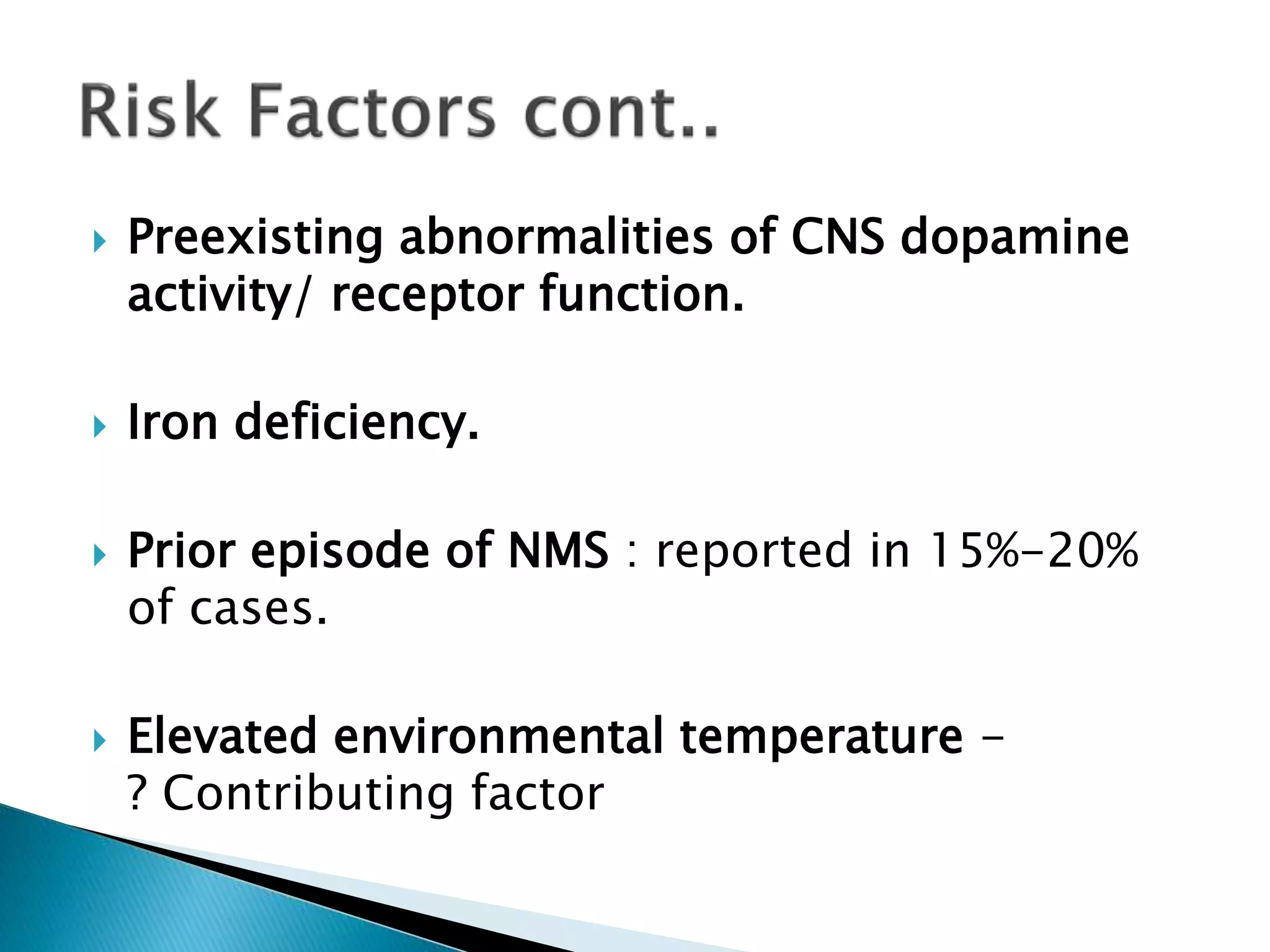

















The document discusses Neuroleptic Malignant Syndrome (NMS), a severe and potentially life-threatening disorder associated with antipsychotic medications, characterized by symptoms such as muscle rigidity, altered mental status, and autonomic instability. It provides information on incidence rates, diagnostic criteria, associated complications, management strategies including supportive care and pharmacological interventions, as well as risk factors for development. The document highlights the importance of early recognition and intervention to mitigate complications and improve outcomes.























































































