In this ppt I have tried to give basic idea about Diabetic peripheral and autonomic neuropathy ..from Levine textbook,IWGDF guideline etc
Hope it will b helpful for trainee and physician
DIABETIC NEUROPATHY
Diabeticneuropathies are serious, chronic complications of diabetes with
diverse clinical manifestations.
Identified in patients with Prediabetes
i. Type 1 diabetes mellitus
ii. Type 2 diabetes mellitus
3.
Classification of DiabeticNeuropathies
Generalized Symmetrical Polyneuropathies
Distal sensory or sensorimotor polyneuropathy
Small – fiber neuropathy
Autonomic neuropathy
Large - fiber sensory neuropath
Focal and Asymmetrical Neuropathy
Cranial neuropathy (single or multiple)
Truncal neuropathy (thoracic radiculopathy)
Limb mononeuropathy (single or multiple)
Lumbosacral radiculoplexopathy (amyotrophy, proximal neuropathy)
Combinations
Polyradiculoneuropathy
Diabetic neuropathic cachexia
Dr Pankaj Patawari
4.
COMMON RISK FACTORS
Duration of Diabetes Mellitus
4-10% by 5 years / up to 50% by 25 years
Control of Sugar status
Smoking and Alcohol consumption
Tobacco use
Induces vasoconstriction and nerve ischemia
Age
Male gender
Damage to the blood vessels
Hyperlipidemia
Mechanical Injury
Overweight status
Genetic susceptibility
Dr Pankaj Patawari
5.
Causes/Differential
Distal axonal neuropathies
Vitamin B12 deficiency
Monoclonal gammopathies
Vasculitis
Infectious causes
Lymphoproliferative disorders
Paraneoplastic diseases
Small fiber neuropathies (many of these neuropathies)
Alcoholism
HIV
Monoclonal gammopathy
Phamacologic or environmental toxins
Sjogren Syndrome
Systemic or familial amyloidosis
Sarcoidosis
Hereditary sensory neuropathy
Other inherited neuropathies
Demyelinating neuropathies
Chronic inflammatory demyelinating polyradiculoneuropathy and other demyelinating neuropathies
Multifocal neuropathy
Other causes of mono neuropathy multiplex
Radiculopathy and plexopathies
Sarcoidosis
Amyloidosis
Vasculitis
Neoplastic and paraneoplastic causes
6.
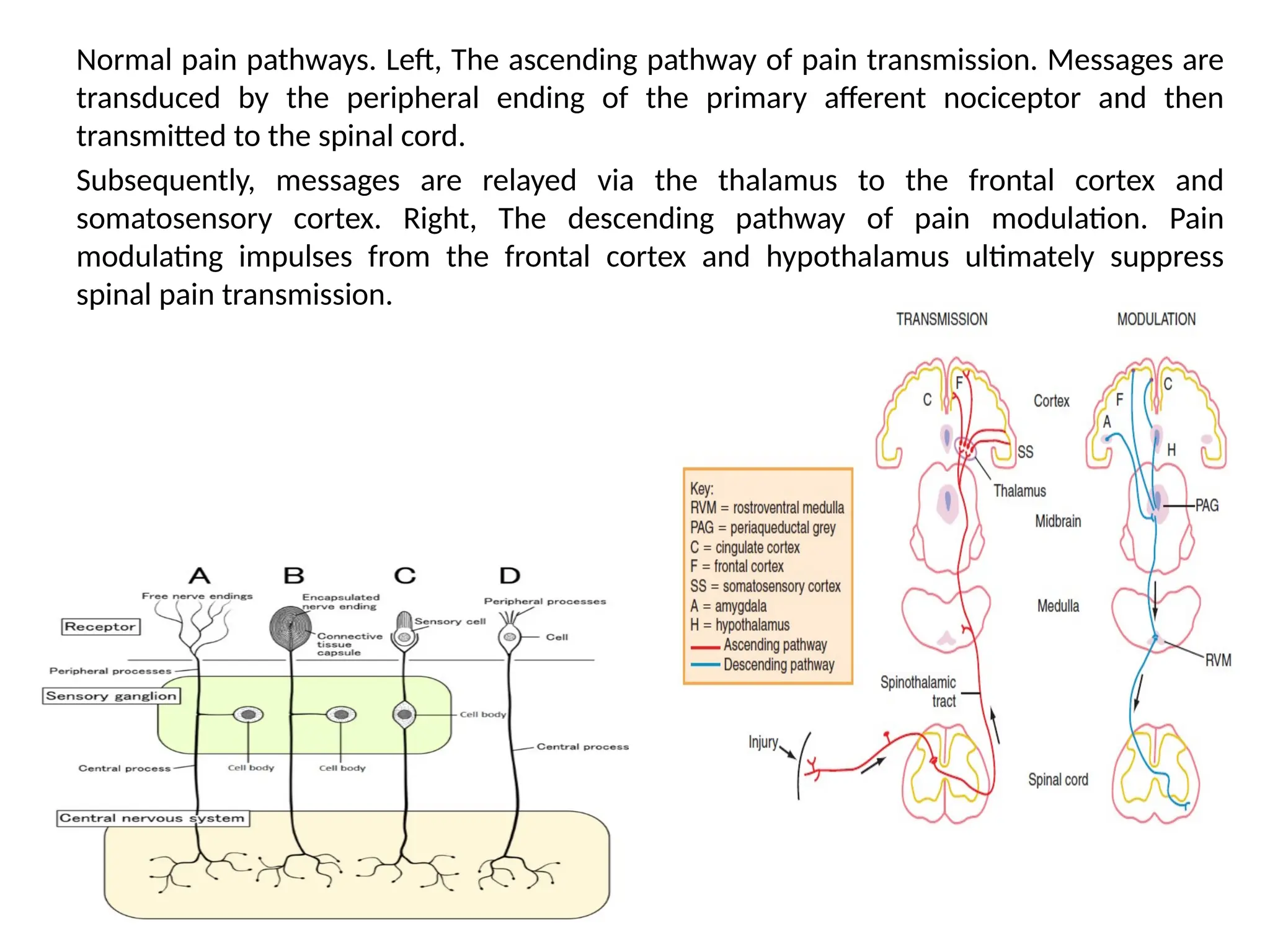
Normal pain pathways.Left, The ascending pathway of pain transmission. Messages are
transduced by the peripheral ending of the primary afferent nociceptor and then
transmitted to the spinal cord.
Subsequently, messages are relayed via the thalamus to the frontal cortex and
somatosensory cortex. Right, The descending pathway of pain modulation. Pain
modulating impulses from the frontal cortex and hypothalamus ultimately suppress
spinal pain transmission.
7.
THREE TYPES OFPAIN
The proposed etiologies of the different types.
a. Dysesthesia pain - Increases firing of damaged or abnormally excited nociceptive fibers, particularly sprouting
regenerating fibers in the cutaneous tissue.
b. Paresthesia pain - Spontaneous activity and increased mechanosensitivity near the cell body of damaged afferents in the
dorsal root ganglion.
c. Paresthesia pain - Ectopic impulses generated from demyelinated patches of myelinated axons.
d. Muscular pain - Ectopic impulses to the muscle generated from demyelinated patches resulting in muscle spasms and
pain.
e. Paresthesia pain - Loss of large myelinated fibers on the effects of the small unmyelinated fibers (modified gate control
hypothesis). Pain signals are transmitted from the spinal cord pain transmission neuron as a result of the input from the
unmyelinated, myelinated, and inhibitor cells.
f. Paresthesia pain – Increased firing of endings of nociceptive afferents that innervate the nerve sheaths themselves (nervi
nervorum). The endoneurial swelling is secondary to endoneurial sodium accumulation and marked nerve hydration.
g. Muscular pain - Reflex loop (Livingston’s vicious cycle) involving a nociceptive input that activates the motor neuron within
the spinal cord causing muscle spasms that in turn activate the muscle nociceptors and feeds back to the spinal cord to
sustain the spasm.
9.
The Consensus DevelopmentConference on Standardized Measures in Diabetic
Neuropathy recommended the following five measures to be employed in the
diagnosis of diabetic neuropathy:
1 clinical measures;
2 morphological and biochemical analyses;
3 electrodiagnostic assessment;
4 quantitative sensory testing;
5 autonomic nervous system testing.
1 Clinical measures
Clinical measures include the following:
1 general medical history and neurological history;
2 neurological examination which consists of:
a sensory (pain, light touch, vibration, position);
b motor (graded as normal = 0, weak = 1–4);
c reflex (present or absent);
d autonomic examination (bedside tests including heart rate variation
during deep breathing and postural blood pressure response).
10.
Causes for DSPNother than diabetes and referral for a detailed neurological
work-up -
pronounced asymmetry of the neurological deficits;
predominant motor deficits, mononeuropathy, cranial nerve involvement;
rapid development or progression of the neuropathic impairments;
progression of the neuropathy despite optimal glycemic control;
development of symptoms and deficits only in the upper limbs;
family history of non-diabetic neuropathy;
diagnosis of DSPN cannot be ascertained by clinical examination.
11.
Neurological examination
1-MONOFILAMENT TEST
•Each monofilament is marked with a number that represents the decimal
log of 10 times the force in milligrams ranging from 1.65 (000.45 g) to 6.65
(447 g) of linear
• The thicker (higher the number) the monofilament, the more force is
required to cause the buckle.
• Patients without neuropathy should be able to sense the 3.61
monofilament (equivalent to 0.4 gram of linear force).
• The inability to sense monofilaments of 4.17 (equivalent of 1 gram of linear
pressure) or higher is considered consistent with neuropathy (large fiber
modality).
• Inability to sense a monofilament of 5.07 (equivalent to 10 grams of linear
force) is consistent with severe neuropathy and loss of protective
sensation.
12.
10g (5.07) Semmes-Weinsteinmonofilament
Test 3 different sites (ADA-4 sites)
duration-2s
Don’t use for the next 24 hours after assessing 10-15 patients and replacing it after
using it on 70-90 patients
13.
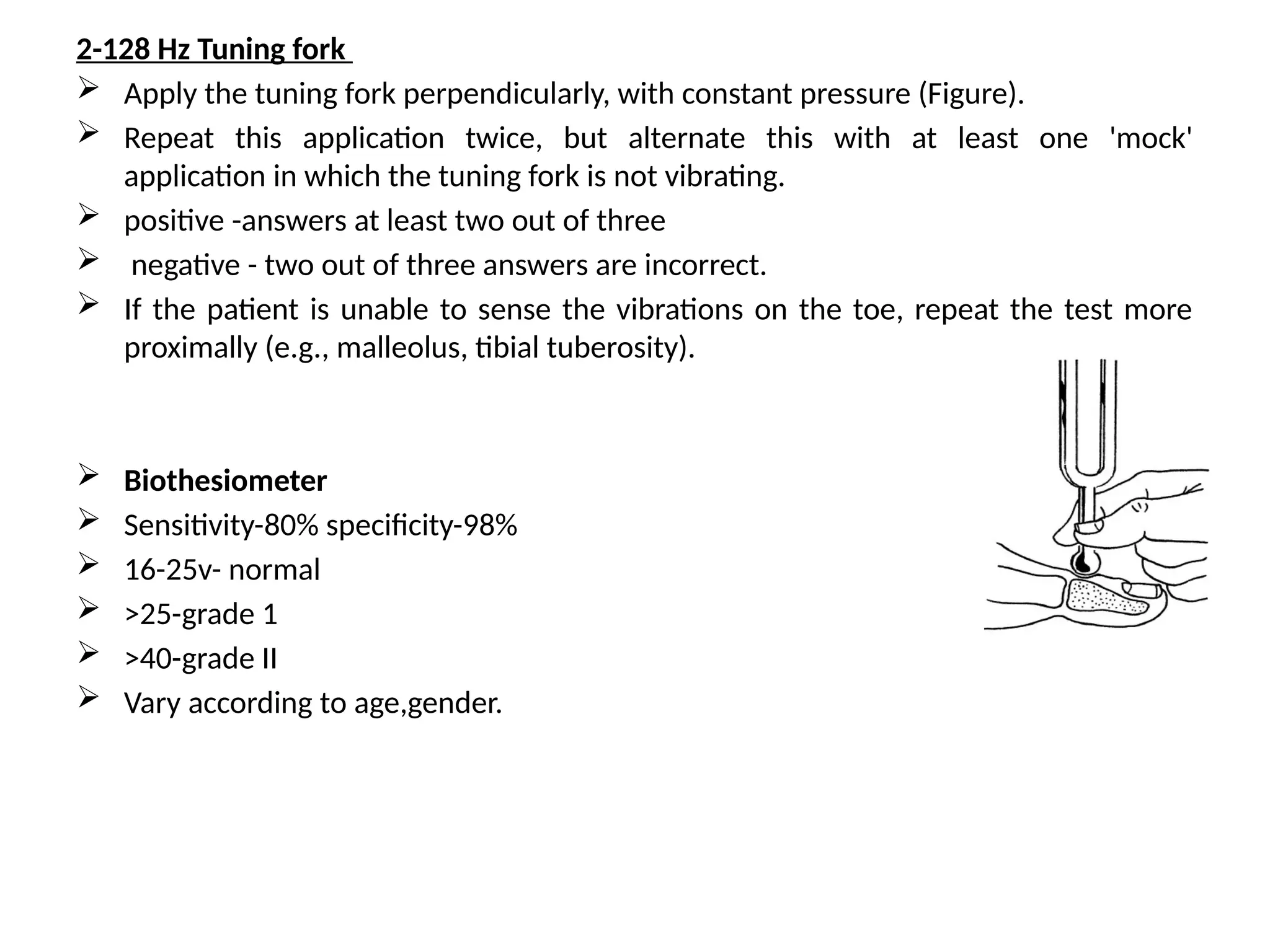
2-128 Hz Tuningfork
Apply the tuning fork perpendicularly, with constant pressure (Figure).
Repeat this application twice, but alternate this with at least one 'mock'
application in which the tuning fork is not vibrating.
positive -answers at least two out of three
negative - two out of three answers are incorrect.
If the patient is unable to sense the vibrations on the toe, repeat the test more
proximally (e.g., malleolus, tibial tuberosity).
Biothesiometer
Sensitivity-80% specificity-98%
16-25v- normal
>25-grade 1
>40-grade II
Vary according to age,gender.
14.
3 Light touchtest
This simple test (also called the Ipswich Touch test) can be used to screen for
loss of protective sensation (LOPS),
The examiner lightly sequentially touches with the tip of hers/his index
finger the tips of the first, third, and fifth toes of both feet for 1–2 s
When touching, do not push, tap, or poke
LOPS is likely when light touch is not sensed in ≥ 2 sites
15.
3-Electrodiagnostic
Differentiate ,localisation oflesion.
Limitations
1 measure only function in the largest, fastest
conducting myelinated fibers;
2 have relatively low specificity in detecting
diabetic neuropathy;
3 show relatively high intra-individual variability
for certain parameters (amplitudes);
4 are vulnerable to external factors such as
electrode locations or limb temperature;
5 provide only indirect information about
symptoms and deficits.
16.
2. Morphological assessment
Suralnerve biopsy
not routinely used
Used when in doubt
Limitation-it may result in complication
Skin biopsy
3-mm punch skin biopsy at the distal leg and quantifying the linear density
of intra-epidermal nerve fiber in at least three 50-μm thick sections per
biopsy, fixed in 2% PLP or Zamboni’s solution, by bright-field
immunohistochemistry or immunofluorescence with anti-protein gene
product 9.5 antibodies (PGP 9.5)
Quantification of intra-epidermal nerve fiber density closely correlated
with warm- and heat-pain threshold,
The diagnostic efficiency and predictive values of this technique were very
high
17.
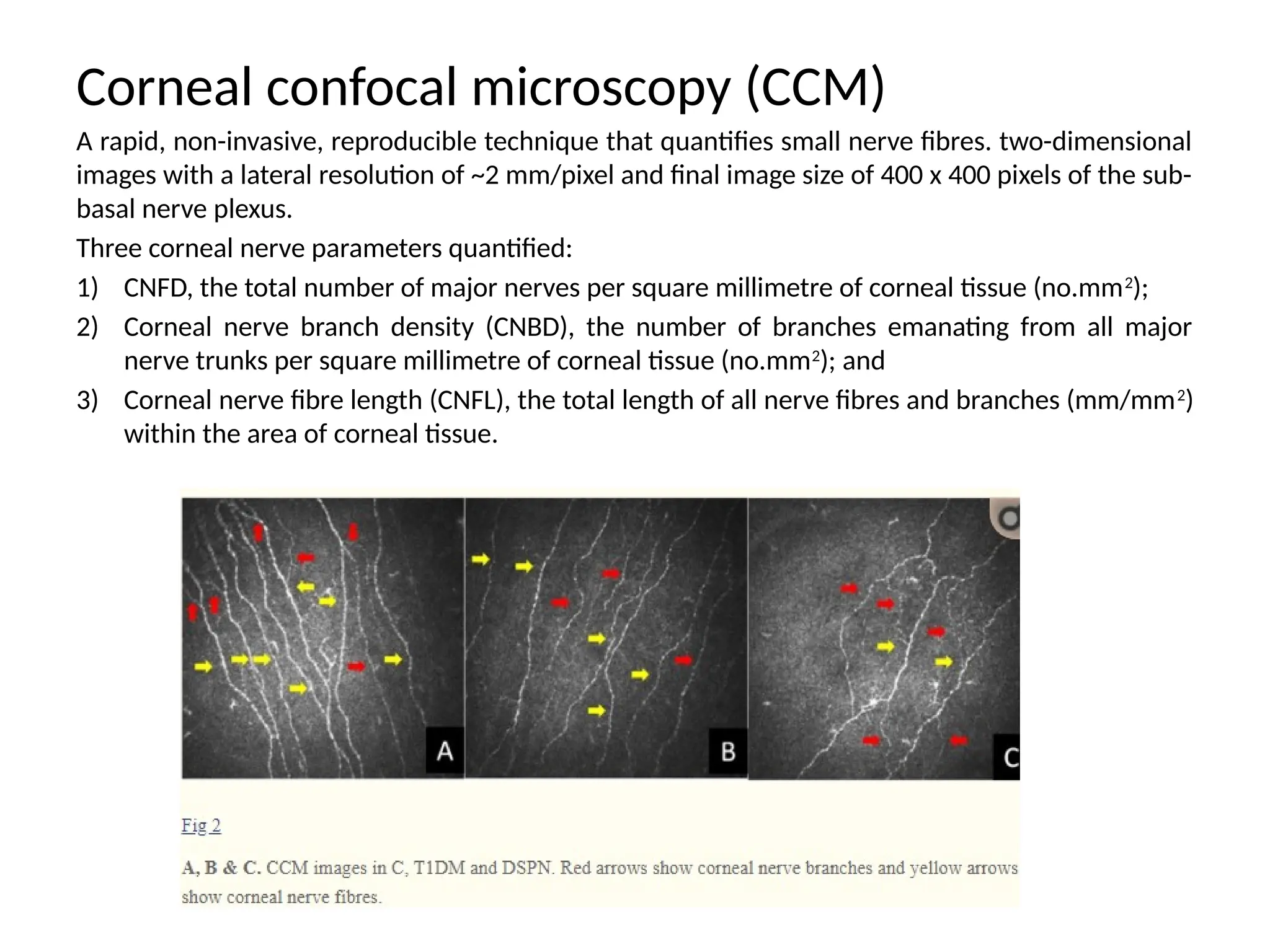
Corneal confocal microscopy(CCM)
A rapid, non-invasive, reproducible technique that quantifies small nerve fibres. two-dimensional
images with a lateral resolution of ~2 mm/pixel and final image size of 400 x 400 pixels of the sub-
basal nerve plexus.
Three corneal nerve parameters quantified:
1) CNFD, the total number of major nerves per square millimetre of corneal tissue (no.mm2
);
2) Corneal nerve branch density (CNBD), the number of branches emanating from all major
nerve trunks per square millimetre of corneal tissue (no.mm2
); and
3) Corneal nerve fibre length (CNFL), the total length of all nerve fibres and branches (mm/mm2
)
within the area of corneal tissue.
DISTAL SYMMETRICAL POLYNEUROPATHY
Mostcommon form of diabetic neuropathies.
Sensory deficits predominate
Stocking-glove distribution.
Advanced cases, sensation becomes impaired over the anterior chest and
abdomen, producing a truncal wedge-shaped area of sensory loss.
Autonomic symptoms usually correlate with the severity of the neuropathy.
Minor motor involvement affecting the distal muscles of the lower extremities.
2 major subgroups
large-fiber variant
small-fiber variant
OTHER VARIANTS-
DIABETIC POLYRADICULONEUROPATHY
Often begins as a distal symmetrical polyneuropathy
Later involves proximal segments of the PNS including multiple lumbosacral roots,
thoracic posterior primary rami, and (less commonly) cervical myotomes.
20.
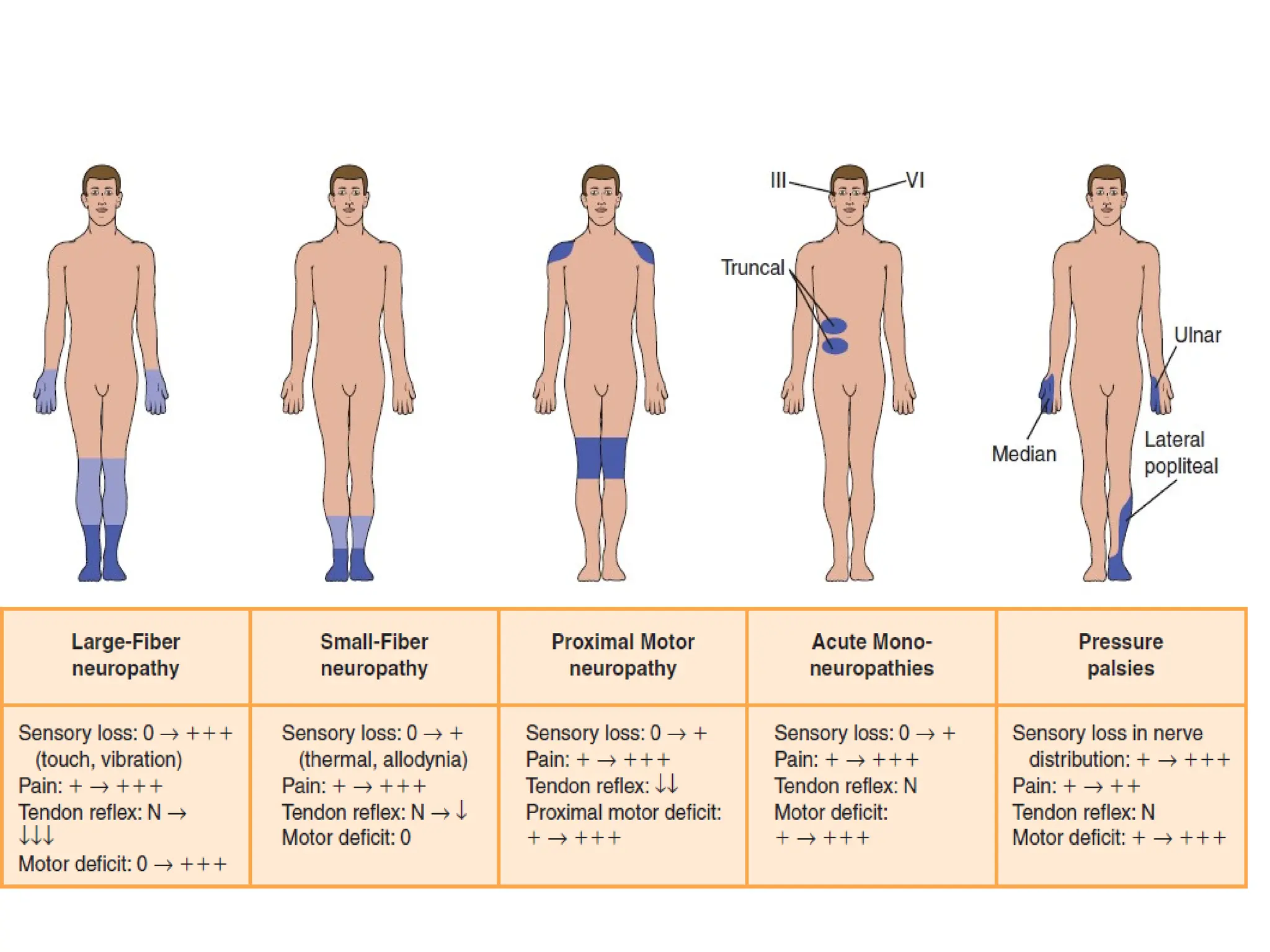
LARGE FIBER NEUROPATHYSMALL FIBER NEUROPATHY
often asymptomatic, but sensory deficit
may be detected by careful examination
pain of a deep, burning, stinging, aching
character, spontaneous shooting pains
paresthesias allodynia to light touch,
impairment of vibration and joint position
sense
Pain and temperature modalities are
impaired, with relative preservation of
vibration and joint position sensation
diminished muscle stretch reflexes muscle stretch reflexes preserved
ataxia may develop -
IMPAIRED GLUCOSE TOLERANCENEUROPATHY
It is now clear that peripheral neuropathy can occur before the onset of clinically
diagnosable diabetes mellitus; this is known as impaired glucose tolerance
neuropathy.
TREATMENT-INDUCED NEUROPATHY
An acute painful neuropathy (burning pain and paresthesias) develop in the distal
lower extremities
Precipitated following initiation of treatment of a diabetic patient with insulin.
Spontaneous resolution to follow.
Pathological studies demonstrate active axonal regeneration, which may act as
generators of spontaneous nerve impulses.
.
23.
DIABETIC NEUROPATHIC CACHEXIA
Acute and severe painful diabetic neuropathy associated with precipitous
severe weight loss, depression, insomnia, and impotence in men.
More common in men with poor glucose control.
NEUROPATHIC ARTHROPATHY
Complication seen in patients with diabetes who often have foot ulcers
and autonomic impairment.
Tends to involve the small joints in the feet.
24.
FOCAL AND ASYMMETRICALNEUROPATHIES
LIMB MONONEUROPATHY
Single mononeuropathies are caused by two basic mechanisms:
a) Nerve infarction: abrupt onset of pain followed by variable weakness and
atrophy.
b) Entrapment: more common than nerve infarctions.
Because the primary pathological lesion results in acute axonal degeneration,
recovery tends to be slow.
The median, ulnar, and fibular nerves are most commonly affected.
The reason diabetes predisposes to nerve entrapment is unknown.
CRANIAL MONONEUROPATHIES
A third nerve palsy is the most common.
Pupillary sparing, the hallmark of diabetic third-nerve palsy, results from ischemic
infarction of the centrifascicular oculomotor axons due to diabetic vasculopathy of
the vasa nervorum.
The peripherally located pupillary motor fibers are spared as a result of collateral
circulation from the circumferential arteries.
With decreasing frequency, the fourth, sixth, and seventh nerves are also affected.
25.
TRUNCAL NEUROPATHY
InvolvesT4 - T12 spinal nerve roots.
Causes pain (burning, stabbing, boring, belt like pain ) or dysesthesias in
areas of the chest or abdomen.
Affecting either the entire dermatomal distribution of adjacent spinal
nerves or, restricted areas limited to the distribution of the dorsal or
ventral rami of spinal nerves.
Bulging of the abdominal wall as a result of weakness of abdominal
muscles may also occur.
Contact with clothing can be very unpleasant.
The onset may be either abrupt or gradual.
The symptoms may persist for several months before gradual and
spontaneous resolution within 4 to 6 months.
Focal anhidrosis on the trunk correlating with the area of pain is detected
with the help of the thermoregulatory sweat test.
26.
MULTIPLE MONONEUROPATHIES
Involvementof two or more nerves.
Onset is abrupt in one nerve, and then other nerves are involved sequentially at
irregular intervals.
Nerve infarction results from occlusion of the vasa nervorum.
DIABETIC AMYOTROPHY / BRUNS GARLAND SYNDROME
This is debilitating, painful, asymmetrical motor neuropathy with profound atrophy
of proximal leg muscles.
Pain usually recedes spontaneously long before motor strength begins to improve.
Involvement of multiple nerve roots or proximal nerve segments.
Almost always restricted to the lower limbs. In some patients, additional body
region is also affected, mostly the thoracic occasionally cervical region.
Although a beneficial effect of immunomodulating therapies has been proposed,
controlled studies have shown no positive effect for corticosteroids in enhancing
the recovery of the motor deficit.
Recovery takes up to 24 months because of the slow rate of axonal regeneration.
27.
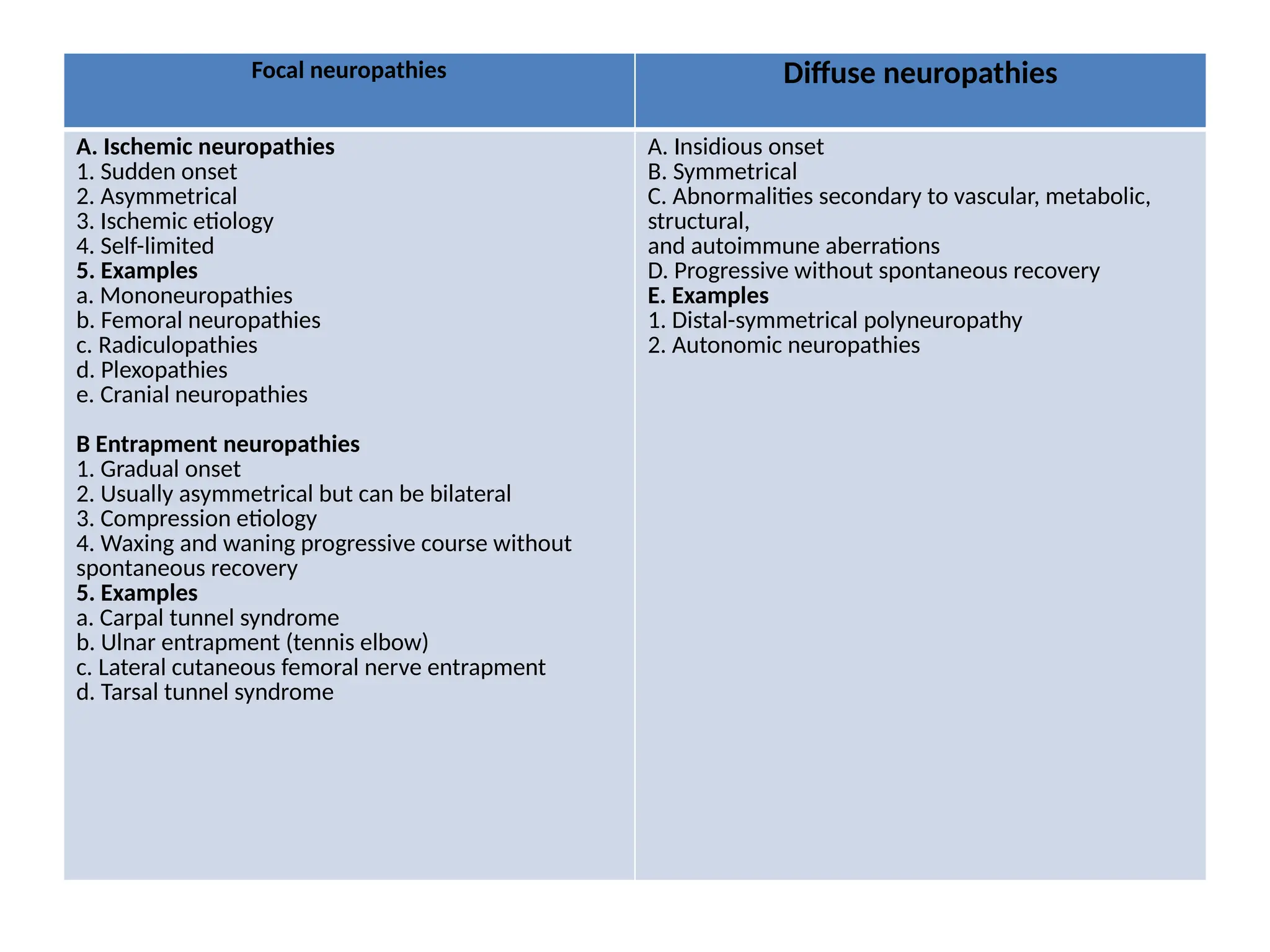
Focal neuropathies Diffuseneuropathies
A. Ischemic neuropathies
1. Sudden onset
2. Asymmetrical
3. Ischemic etiology
4. Self-limited
5. Examples
a. Mononeuropathies
b. Femoral neuropathies
c. Radiculopathies
d. Plexopathies
e. Cranial neuropathies
B Entrapment neuropathies
1. Gradual onset
2. Usually asymmetrical but can be bilateral
3. Compression etiology
4. Waxing and waning progressive course without
spontaneous recovery
5. Examples
a. Carpal tunnel syndrome
b. Ulnar entrapment (tennis elbow)
c. Lateral cutaneous femoral nerve entrapment
d. Tarsal tunnel syndrome
A. Insidious onset
B. Symmetrical
C. Abnormalities secondary to vascular, metabolic,
structural,
and autoimmune aberrations
D. Progressive without spontaneous recovery
E. Examples
1. Distal-symmetrical polyneuropathy
2. Autonomic neuropathies
28.
TREATMENT
Despite major advancesin diabetes treatment in general, to date, there is a
paucity of U.S. Food and Drug Administration–approved therapies that
effectively target reversal of the underlying nerve damage.
29.
Attempts to treatdiabetic neuropathy by manipulating nerve metabolism
have been disappointing.
Clinical trials of myoinositol supplementation have shown conflicting
results
Results of aldose reductase inhibitors have so far failed.
Neurotrophin treatments for diabetic neuropathy, such as nerve growth
factor, have been disappointing
Adverse Effects
Amitriptyline –Common Adverse Effects
Xerostomia, Somnolence, Fatigue, Headache, Dizziness, Insomnia, Orthostatic hypotension, Anorexia, Nausea,
Urinary retention, Constipation, Blurred vision, Accommodation, Disturbance, Mydriasis, Weight gain.
Major Adverse Effects
Delirium, Cardiac arrhythmias, Conduction abnormalities, Myocardial infarction, Heart failure exacerbation,
Stroke, Seizures, Hepatotoxicity, Bone marrow suppression, Suicidal thoughts and behavior, Shift to mania in
bipolar disorder, Neuroleptic malignant syndrome, Serotonin syndrome, Severe hyponatremia, Fragility bone
fractures .
Duloxetine – Common Adverse Effects
Nausea, Somnolence, Dizziness, Constipation, Dyspepsia, Diarrhea, Xerostomia, Anorexia, Headache,
Diaphoresis, Insomnia, Fatigue, Decreased libido.
Major Adverse Effects
Stevens-Johnson syndrome, Hepatotoxicity, Hypertensive crisis, Gastrointestinal hemorrhage, Delirium,
Myocardial infarction, Cardiac arrhythmias, Glaucoma, Suicidal thoughts and behavior, Shift to mania in
patients with bipolar disorder, Seizures, Severe hyponatremia, Fragility bone fractures, Serotonin syndrome,
Neuroleptic malignant syndrome
33.
Pregabaline – CommonAdverse Effects
Somnolence, Dizziness, Peripheral edema, Headache, Ataxia, Fatigue, Xerostomia, Weight gain
Major Adverse Effects
Angioedema, Hepatotoxicity, Rhabdomyolysis, Suicidal thoughts and behavior, Seizures after rapid
discontinuation, Thrombocytopenia.
Gabapentine – Common Adverse Effects
Somnolence, Dizziness, Ataxia, Fatigue.
Major Adverse Effects
Stevens-Johnson syndrome, Suicidal thoughts and behavior, Seizures after rapid discontinuation.
35.
Non pharmacological treatment
Psychological support
Physical measures
Accupuncture
Transcutaneous electrical nerve stimulation (TENS)
External muscle stimulation (high-tone therapy)
Frequency-modulated electromagnetic nerve stimulation (FREMS)
Electrical spinal cord stimulation
Surgical decompression
MOST IMPORTANT OF ALL - “Diabetic Neuropathy is The Presence Of Symptoms And/Or Signs Of
Peripheral Nerve Dysfunction In People With Diabetes After The Exclusion Of Other Causes”
BoultonAJM, Gries FA, Jervell JA: Guidelines for the diagnosis and outpatient management of
diabetic peripheral neuropathy. Diabetic Med 15:508–514, 1998
“Also 10-55% patients with diabetic neuropathies may have other conditions that cause similar
manifestations- CIDP, vitamin B12 deficiency, alcoholic neuropathy etc”
Dyck PJ, Kratz KM, Karnes JL, Litchy WJ, Klein R, Pach JM, Wilson DM, O'BrienPC, Melton LJ 3rd,
Service FJ. The prevalence by staged severity of various types of diabetic neuropathy,
retinopathy, and nephropathy in a population-based cohort: the Rochester Diabetic Neuropathy
Study. Neurology. 1993 Apr;43(4):817-24.
36.
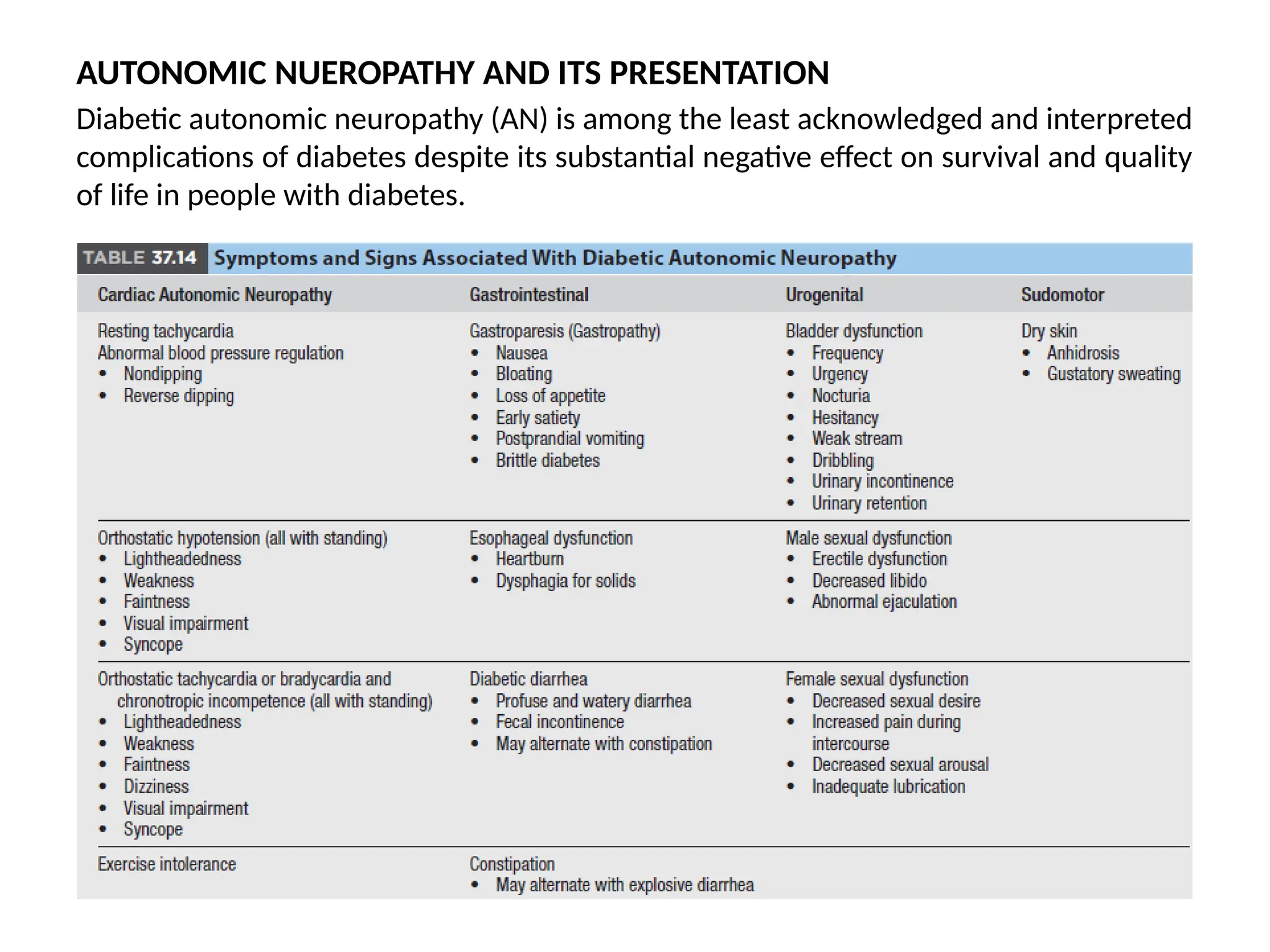
AUTONOMIC NUEROPATHY ANDITS PRESENTATION
Diabetic autonomic neuropathy (AN) is among the least acknowledged and interpreted
complications of diabetes despite its substantial negative effect on survival and quality
of life in people with diabetes.
37.
Hypoglycaemia unawareness: Thoughliterature has shown negative correlation of AN
with hypoglycaemia unawareness, recent evidence has shown attenuation of
epinephrine release with hypoglycaemia and blunted response and release of plasma
pancreatic polypeptidase in patients with AN
Hypoglycaemic autonomic failure: Attenuation of epinephrine and other counter
regulatory hormones in patients with hypoglycaemia unawareness is defined as
hypoglycaemic autonomic failure. Presence of AN further attenuates this response and
increases the severity of this incidence. The strict glycaemic control aggravates
hypoglycaemic autonomic faillure.
Impaired microvascular blood flow to the skin:
Microvascular insufficiency results in abnormal contraction of the arterioles and
arteries of the skin.
Laser Doppler flowmetry is a non-invasive method of assessing the changes in
microvascular blood flow with mental arithmetic, cold pressor, heating, and
handgrip.
Dry skin leading to fissures and ulcer development helps in further seedling of
infection and gangrene.
AN also causes increased osteoclastic activity and reduced bone density.
CORNERSTONES OF FOOTULCER PREVENTION
There are five key elements that underpin efforts to prevent foot ulcers:
1. Identifying the at-risk foot
2. Regularly inspecting and examining the at-risk foot
3. Educating the patient, family and healthcare professionals
4. Ensuring routine wearing of appropriate footwear
5. Treating risk factors for ulceration
1-Identifying the at-risk foot-
History: Previous ulcer/lower extremity amputation, claudication
• Vascular status: palpation of pedal pulses
• Loss of protective sensation (LOPS): assess with one of the following techniques
(see addendum for details):
- Pressure perception: Semmes-Weinstein 10 gram monofilament
- Vibration perception: 128 Hz tuning fork
- When monofilament or tuning fork are not available test tactile sensation: lightly touch the
tips of the toes of the patient with the tip of your index finger for 1–2 seconds
44.
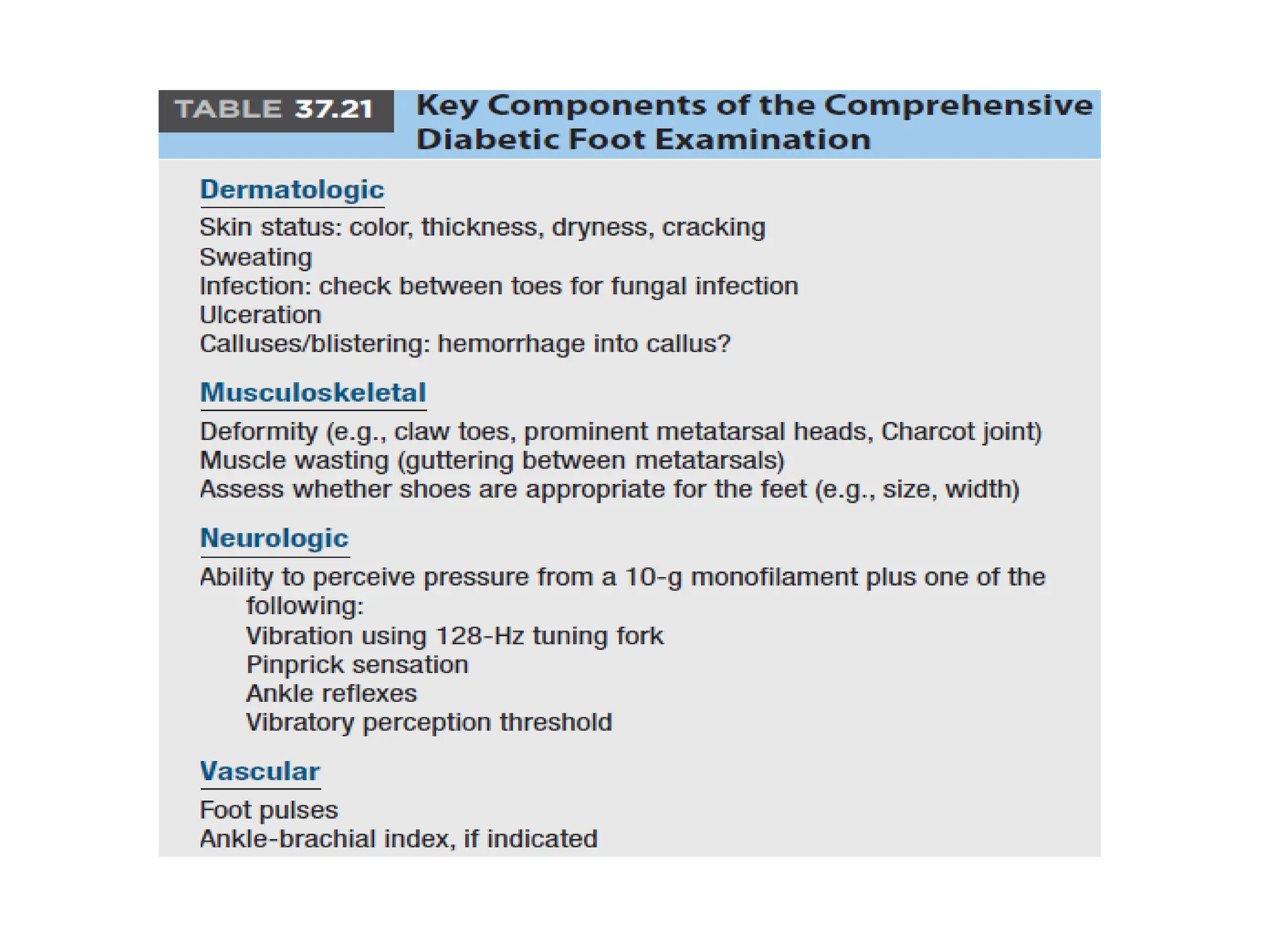
2. Regularly inspectingand examining the at-risk foot (IWGDF risk 1 or higher)
In a person with diabetes with loss of protective sensation or peripheral artery disease (IWGDF
risk 1-3) perform a more comprehensive examination, including the following:
• History: inquiring about previous ulcer/lower extremity amputation, end stage renal disease,
previous foot education, social isolation, poor access to healthcare and financial constraints, foot
pain (with walking or at rest) or numbness, claudication
• Vascular status: palpation of pedal pulses
• Skin: assessing for skin colour, temperature, presence of callus or oedema, pre-ulcerative signs
• Bone/joint: check for deformities (e.g., claw or hammer toes), abnormally large bony prominences,
or limited joint mobility. Examine the feet with the patient both lying down and standing up
• Assessment for loss of protective sensation (LOPS), if on a previous examination protective
sensation was intact
• Footwear: ill-fitting, inadequate, or lack of footwear.
• Poor foot hygiene, e.g. improperly cut toenails, unwashed feet, superficial fungal infection, or unclean
socks
• Physical limitations that may hinder foot self-care (e.g. visual acuity, obesity)
• Foot care knowledge
45.
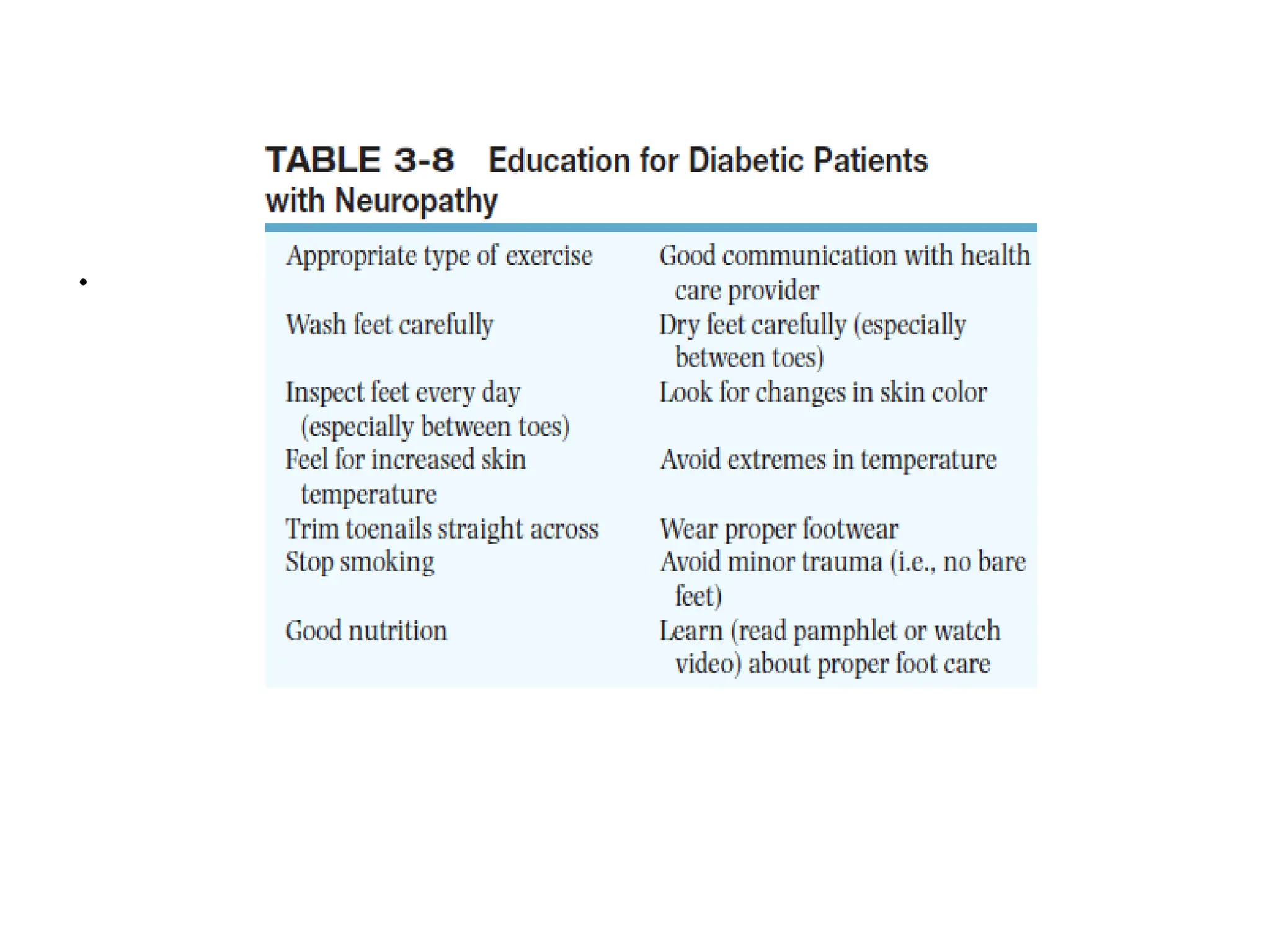
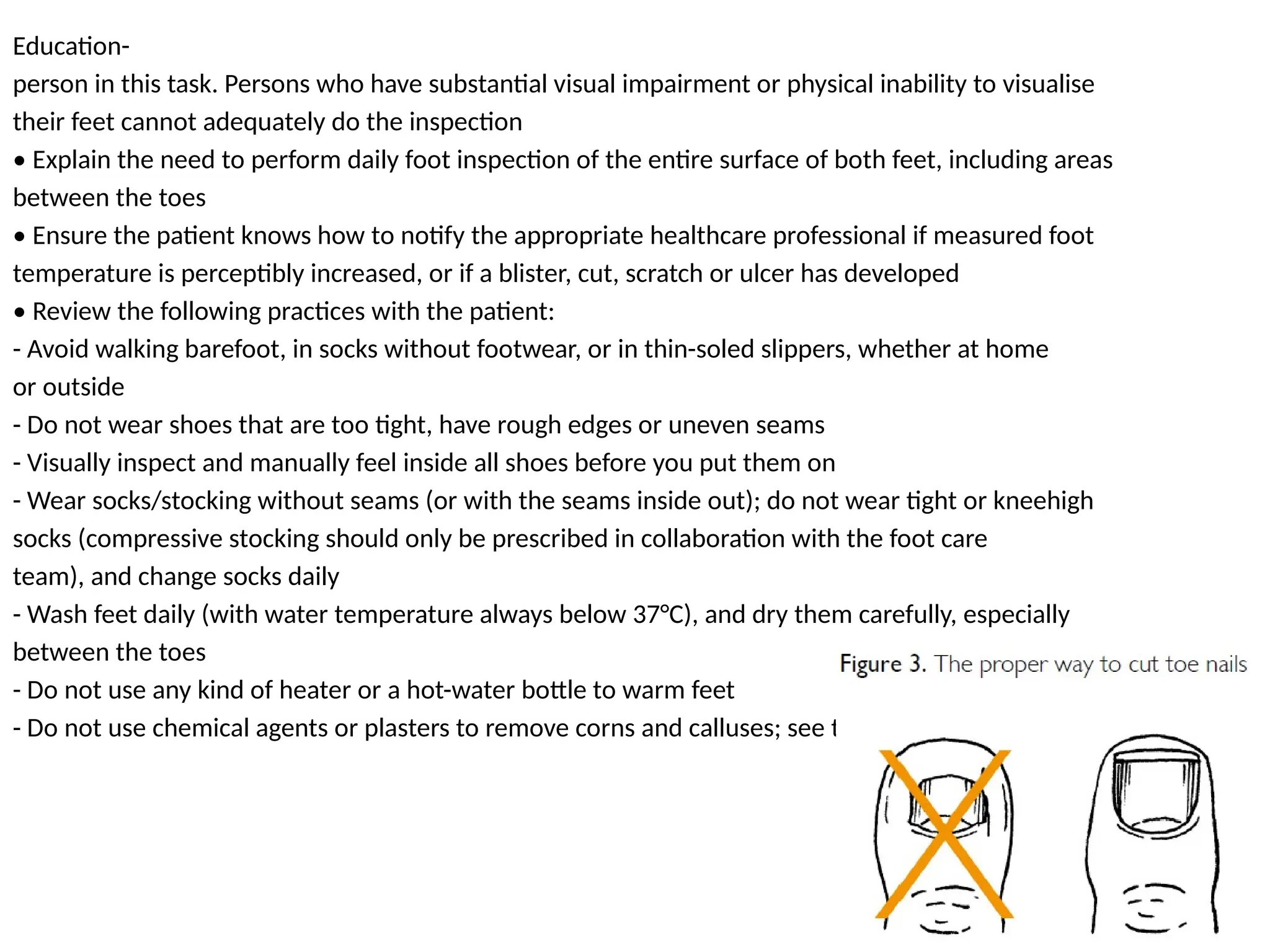
Education-
person in thistask. Persons who have substantial visual impairment or physical inability to visualise
their feet cannot adequately do the inspection
• Explain the need to perform daily foot inspection of the entire surface of both feet, including areas
between the toes
• Ensure the patient knows how to notify the appropriate healthcare professional if measured foot
temperature is perceptibly increased, or if a blister, cut, scratch or ulcer has developed
• Review the following practices with the patient:
- Avoid walking barefoot, in socks without footwear, or in thin-soled slippers, whether at home
or outside
- Do not wear shoes that are too tight, have rough edges or uneven seams
- Visually inspect and manually feel inside all shoes before you put them on
- Wear socks/stocking without seams (or with the seams inside out); do not wear tight or kneehigh
socks (compressive stocking should only be prescribed in collaboration with the foot care
team), and change socks daily
- Wash feet daily (with water temperature always below 37°C), and dry them carefully, especially
between the toes
- Do not use any kind of heater or a hot-water bottle to warm feet
- Do not use chemical agents or plasters to remove corns and calluses; see the appropriate
Editor's Notes
#11 Proposed
etiologies of diffuse diabetic
neuropathy. Abnormal vasa
nervorum, insulin deficiency,
hyperglycemia, abnormal fatty
acid metabolism, increased
polyol activity, decreased nerve
myo-inositol, increased
glycosylation of neural proteins,
and neural autoantibodies have
all been suggested as etiologies
of diabetic neuropathy. There
appears to be a common end
result: confirmed clinical
neuropathy. In a single individual,
one or more of these pathways
may be prominent. In another
individual, other pathways may
play a more predominant role.
#15 This table lists 20 of the
24 Semmes-Weinstein monofilaments by size and grams of linear
force. The most important calibrations: 3.61, 431, 4.56, 5.07 and
6.65 are marked (✪). Commercially available kits of six typically
include these plus the 2.83 evaluator size.
Patients who are able to sense the 3.61 size (0.4 grams of
force) are presumed not to have small fiber neuropathy. Patients
who are able to sense the 5.07 monofilament (10 grams target
force) have retained protective sensation even if they have may
have mild small fiber neuropathy. Inability to sense the 5.07 size
is: (1) consistent with severe neuropathy, (2) greatly increases the
possibility of a neuropathic ulcer and (3) is one of the five
indications for custom insoles/footwear for the diabetic patient
(ses text and Pearls).
Monofilaments with an evaluator size smaller than the 3.61 are
primarily utilized for the evaluation of the hands. Evaluation of
sensation of the hands requires different thresholds than those
illustrated for the foot (plantar).
#16 First apply the monofilament on the patient's hands (or elbow or forehead) to demonstrate what the sensation feels like.
Test three different sites on both feet, selecting from those shown in Figure
Ensure the patient cannot see whether or where the examiner applies the filament.
Apply the monofilament perpendicular to the skin surface (Figure a) with sufficient force to cause the filament to bend or buckle (Figure b).
The total duration of the approach -> skin contact -> and removal of the filament should be approximately 2 seconds.
Peripheral neuropathy can be detected using the 10g (5.07 Semmes-Weinstein) monofilament (detects loss of protective sensation) and a tuning fork (128 Hz, detects loss of vibratory sensation).
.
#18 First, apply the tuning fork on the patient's wrist (or elbow or clavicle) to demonstrate what the sensation feels like.
Ensure the patient cannot see whether or where the examiner applies the tuning fork.
Apply the tuning fork to a bony part on the dorsal side of the distal phalanx of the first toe (or another toe if the hallux is absent).
#19 when the 10 gram monofilament or 128 HZ tuning fork is not available. The test has
reasonable agreement with these tests to determine LOPS, but its accuracy in predicting foot ulcers has
not been established.
#44 Dec with age-20-24 yr, 1.17; 25-29, 1.15; 30-34, 1.13; 35-39, 1.12; 40-44, 1.10; 45-49, 1.08; 50-54, 1.07; 55-59, 1.06; 60-64, 1.04; 65-69, 1.03; and 70-75, 1.02