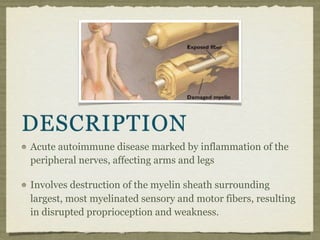
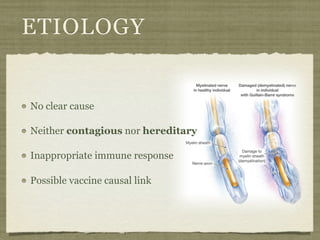
Guillain-Barré syndrome is an acute autoimmune disease marked by inflammation of the peripheral nerves affecting the arms and legs. It involves destruction of the myelin sheath surrounding the largest sensory and motor fibers, resulting in weakness and disrupted proprioception. While the cause is unknown, it is thought to be an inappropriate immune response, possibly linked to certain vaccines. It affects about 2 per 100,000 people annually in a nondiscriminatory manner. Signs and symptoms include numbness, tingling, muscle weakness and diminished reflexes that progress distally. Most patients experience complete recovery within 2 months to 2 years through intravenous immunoglobin therapy or plasmapheresis.