Downloaded 100 times

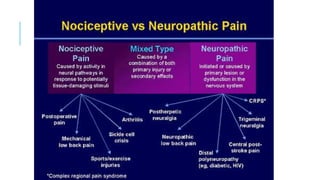
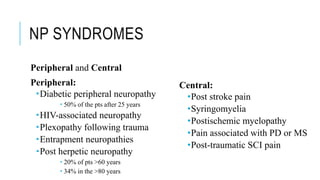
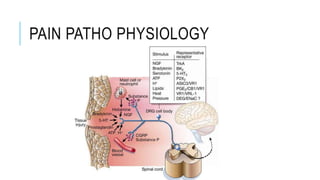
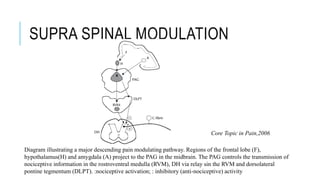
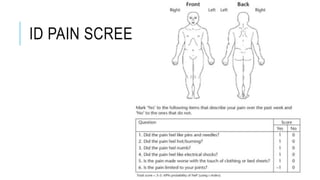


This document discusses neuropathic pain, its definition, symptoms, pathophysiology, assessment, and management. Some key points: - Neuropathic pain is caused by damage or disease affecting the somatosensory nervous system. It is characterized by spontaneous ongoing pain, abnormal sensations, and hypersensitivity. - Common causes include diabetic neuropathy, postherpetic neuralgia, spinal cord injury. Assessment involves history, exam, and tools like LANSS and DN4. - Management includes non-pharmacological options like TENS, physical therapy, as well as drugs like gabapentin, pregabalin, tricyclic antidepressants. - For severe cases, neurosurgical options like cord




























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)






![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)






