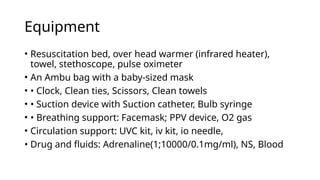
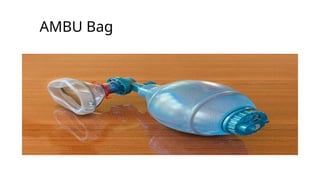
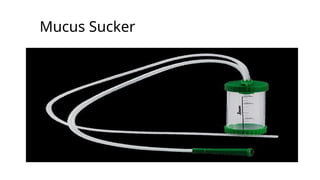
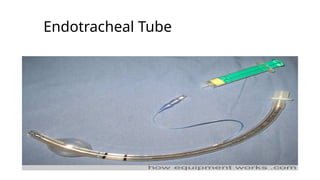
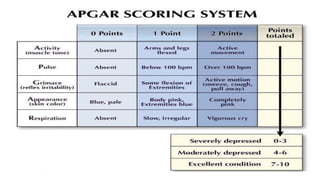
The document discusses neonatal resuscitation, detailing its importance in preventing asphyxia-related deaths at birth and the steps involved, including the use of the Apgar score to assess newborn health. It emphasizes critical preparation and the need for specific equipment during resuscitation, as well as techniques for airway management, breathing support, and chest compressions when necessary. The document also outlines post-resuscitation care and monitoring requirements for infants in order to ensure their health following resuscitation efforts.




















![Bandages and Binders [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/bandagesandbindersautosaved-230314063514-38348509-thumbnail.jpg?width=640&height=640&fit=bounds)

















![Neonatal resuscitation [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/neonatalresuscitationautosaved-210325082037-thumbnail.jpg?width=640&height=640&fit=bounds)
































