Download to read offline

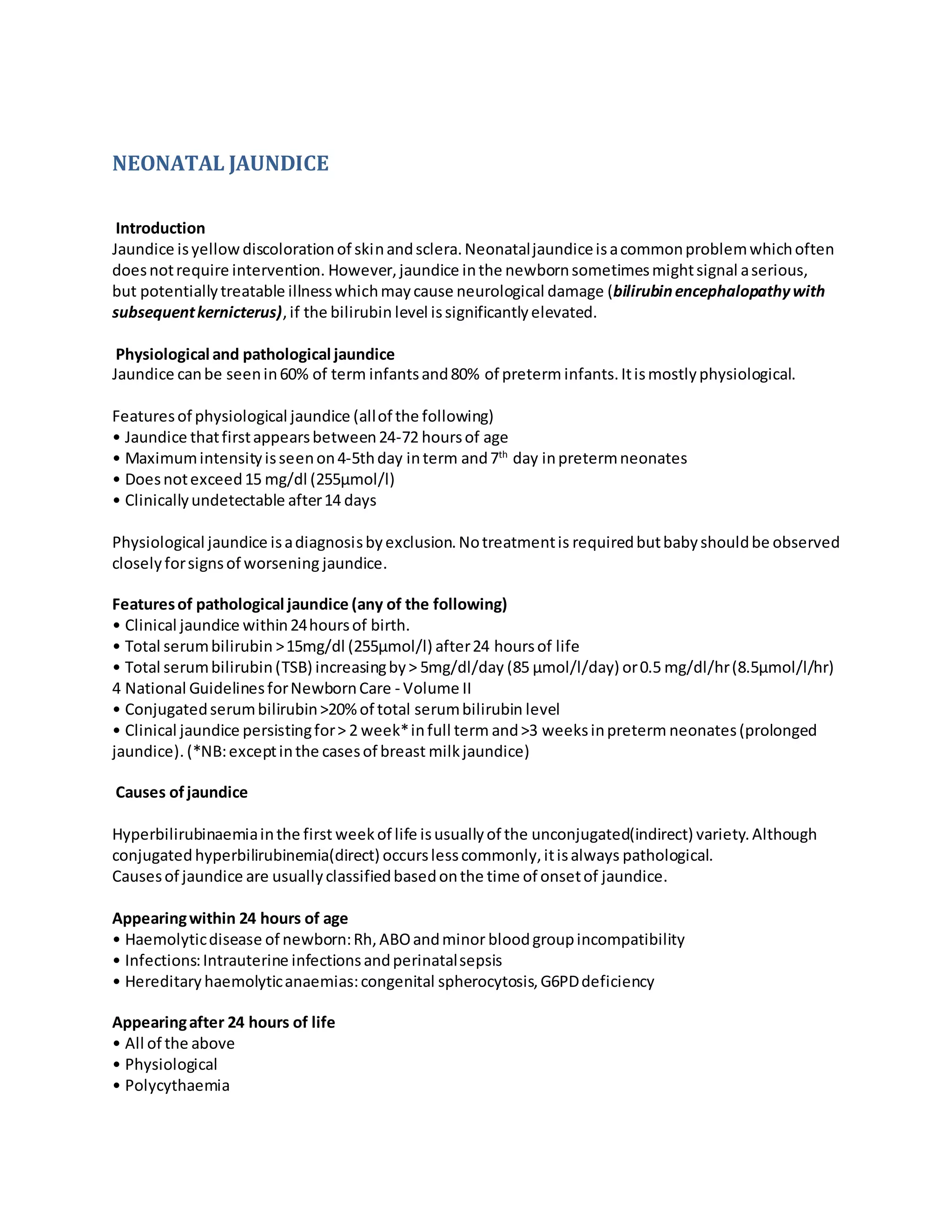







Neonatal jaundice is yellow discoloration of skin and sclera that is common in newborns. It can be physiological or pathological. Physiological jaundice appears between 24-72 hours of age, peaks at days 4-5, does not exceed 15 mg/dl, and is clinically undetectable after 14 days. Pathological jaundice requires further evaluation and may indicate treatable illnesses. Treatment depends on the severity and cause of jaundice, and may involve phototherapy, exchange transfusions, or identifying and treating the underlying condition. Proper assessment and management are needed to prevent neurological damage from severe hyperbilirubinemia.






































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)






![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)









![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)