

















































![Page | 57
Perception
No current hallucinations either visual or auditory. He had paranoid thoughts. No obsessions,
compulsions, and phobias presently.
Cognition
Client was oriented to person, place, time and situation. He was alert and fully oriented presently.
Insight
Poor
Diagnosis - Schizophrenia, undifferentiated type, unspecified pattern
Treatment
In the 1st session patient was just parroting what was said.
In the 2nd session therapist keep some blank papers, coloring pens and crayons on the table and
asked him to draw what he want to express.
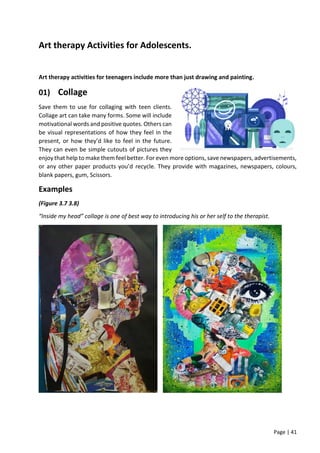
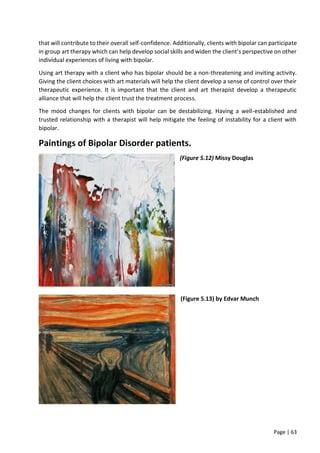
In every session, he was asked to draw what was on his mind at that time. He began to become
more communicative through art. It was in the session, where he first identified figures in his
drawings as being that of his father and mother that the first resistances were set up. His pictures
included his “fears” [Figure 1] and the “bear” which was always hovering about him. This was the
symbol in his life that he had amplified to such a limit that it was controlling his functioning.
Consequently, it had to be controlled. Through therapy an attempt was made to “unfreeze (melt)”
the statue [Figure 2] that he tended to become, and help the screaming child emerge [Figure 1]. He
had to deal with the constant “running away” [Figure 3] from his fears [Figure 4], his abuse, society
[Figures 5 and 6] and learn to face what life had to offer, knowing it is possible [Figure 7].
(Figure 5.1)
Bear hovering over him](https://image.slidesharecdn.com/arttherapy-electivesreport-220531062624-b2a4b0ee/85/Art-Therapy-Electives-Report-pdf-58-320.jpg)








This document provides an overview of art therapy. It defines art therapy and discusses its uses in treating children, adolescents, families, and those with mental disorders. The history of art therapy is traced from its origins in the 1940s. The roles of art therapists and the structure of a typical art therapy session are described. Various art therapy assessments are also mentioned.























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)




![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



