
Downloaded 13 times


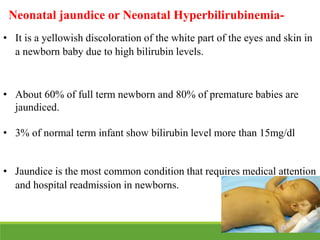
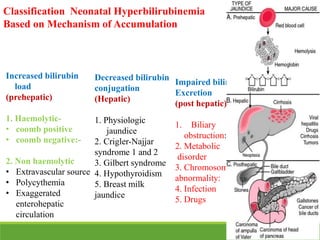
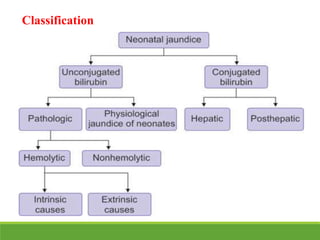
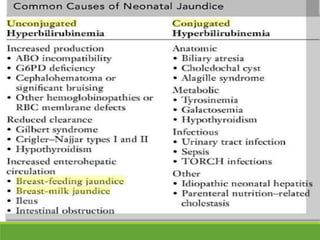

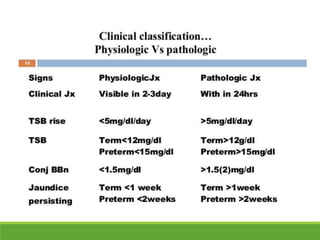

La ictericia neonatal es una condición común en recién nacidos, que se manifiesta como una coloración amarillenta de la piel y los ojos debido a niveles elevados de bilirrubina. Factores como el nacimiento prematuro, hematomas al nacer y la incompatibilidad de grupos sanguíneos pueden aumentar el riesgo de ictericia. Esta condición puede clasificarse como fisiológica o patológica, con diferentes mecanismos y tratamientos necesarios según la causa subyacente.





















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)

