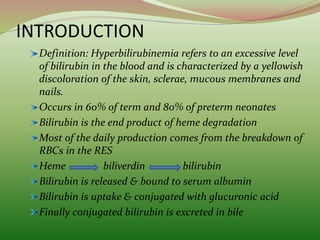
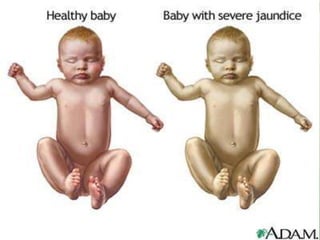
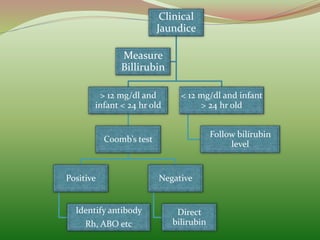
1) Hyperbilirubinemia refers to excessive bilirubin levels in the blood, seen as yellowing of the skin. It occurs commonly in newborns.
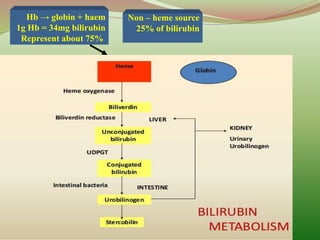
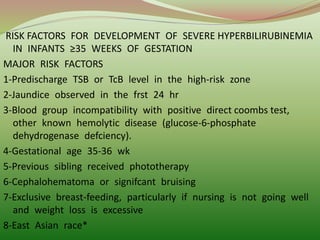
2) Bilirubin is produced from the breakdown of red blood cells. Risk factors for severe hyperbilirubinemia in newborns include blood group incompatibility.
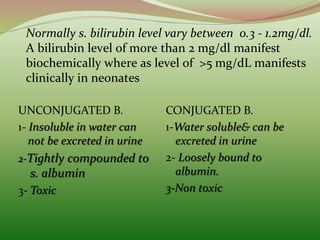
3) Treatment options for high bilirubin levels include phototherapy, which uses light to convert bilirubin into a soluble form excreted in urine, and exchange transfusion, replacing infant blood.