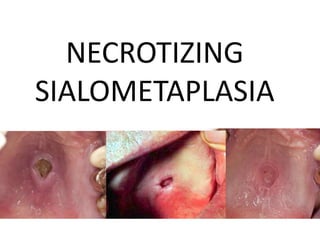
Necrotizing sialometaplasia
•Download as PPTX, PDF•
27 likes•9,276 views

This document discusses necrotizing sialometaplasia, an uncommon condition affecting the salivary glands that is believed to be caused by ischemia and local infarction of salivary tissue. It most frequently presents as a non-ulcerated swelling or pain on the hard palate, and can develop into a crater-like ulcer. Histopathology shows acinar necrosis and squamous metaplasia of salivary ducts. While the cause is unknown, predisposing factors include trauma, dental procedures, tumors, and infections. The condition is self-limiting and typically heals without complications.

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Similar to Necrotizing sialometaplasia
Similar to Necrotizing sialometaplasia (20)
Recently uploaded
Recently uploaded (20)
Necrotizing sialometaplasia
- 2. Necrotizing Sialometaplasia • Uncommon locally destructive inflammatory condition of the salivary glands. • Cause: unknown but they believe it is the result of ischemia of the salivary tissue that leads to local infaction.
- 3. ISCHEMIA AND LOCAL INFARCTION LEADING TO NECROTIZING SIALOMETAPLASIA OXYGEN No blood supply No oxygen No ATP No glucose
- 4. Predisposing factors: –Traumatic injuries –Dental injections –Ill fitting dentures –Upper respiratory infections –Adjacent tumors –Previous tumors ***However many cases occur without any known predisposing factors.
- 5. CLINICAL FEATURES • Most frequently develops in the palatal salivary glands • Hard palate > soft palate ***2/3 of palatal cases are unilateral, with the rest being bilateral or midline in location
- 6. Unilateral
- 8. CLINICAL FEATURES • Has also been reported in other minor salivary gland sites and occasionally in the parotid gland. • Submandibular and sublingual glands are rarely affected.
- 9. CLINICAL FEATURES • Most common in adults and in men • The condition appears initially as a non-ulcerated swelling often associated with pain or paresthesia with crater-like ulcer that can range from less than 1cm to more than 5cm in diameter appearing within 2 to 3 weeks.
- 11. HISTOPATHOLOGIC FEATURES • Microscopic appearance of necrotizing sialometaplasia is characterized by acinar necrosis in early lesions, followed by associated squamous metaplasia of the salivary ducts.
- 13. Treatment • The lesion is self-limiting in most instances and heals uneventfully.
- 14. Xerostomia
- 15. Xerostomia • Refers to subjective sensation of a “dry mouth” • Frequently but not always associated with salivary gland hypofunction.
- 16. Xerostomia
- 17. CAUSES • DEVELOPMENTAL -Salivary gland aplasia • WATER OR METABOLITE LOSS impaired fluid intake -impaired fluid intake -hemorrhage -vomiting or diarrhea
- 18. CAUSES • IATROGENIC -medications • LOCAL FACTORS -decreased mastication -smoking -mouth breathing
- 19. CAUSES • SYSTEMIC DISEASES -Sjogren’s syndrome -diabetes mellitus -diabetes insipidus -sarcoiadosis -HIV infection -Graft-versus-host disease -psychogenic disorder