Download to read offline

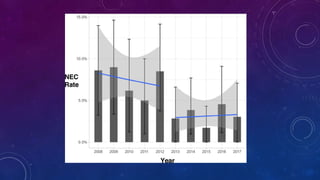
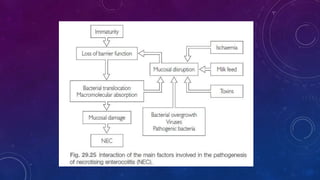
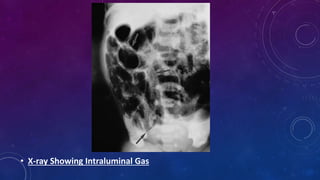


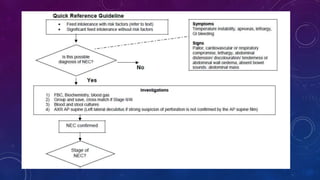
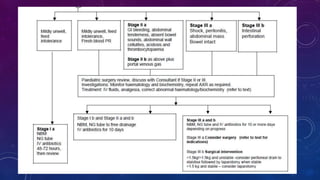


This document provides an overview of necrotizing enterocolitis (NEC), including its epidemiology, risk factors, pathophysiology, clinical features, management, outcomes, prevention and areas for further research. Some key points: - NEC most commonly affects very preterm infants, with a mortality rate around 13% that increases with lower birth weight. - Risk factors include prematurity, hypoxia, poor intestinal integrity, bacterial colonization and enteral feeding. - Clinically it presents with abdominal distension, bloody stools and vomiting. Diagnosis is confirmed via x-ray showing pneumatosis or free air. - Management involves stopping feeds, antibiotics, surgery for complications like perforation.













































































