
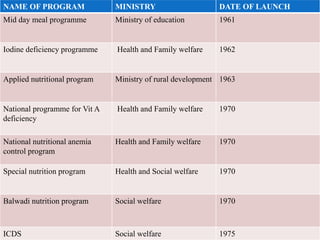











National nutritional programmes for children in India aim to reduce malnutrition, which causes 12% of deaths and 16% disability globally. Key programmes introduced since the 1960s include the mid-day meal scheme providing free lunch to over 100 million schoolchildren, the iodine deficiency programme adding iodine to salt to prevent disorders, and the Integrated Child Development Services programme providing supplementary nutrition, immunization, and education to children and mothers. The programmes have helped reduce morbidity and mortality from malnutrition in India over the decades.










































































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)











