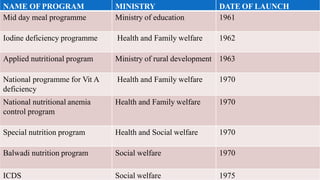
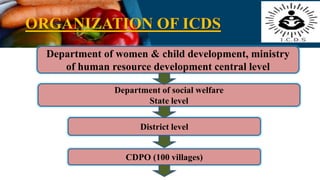
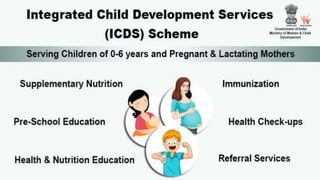
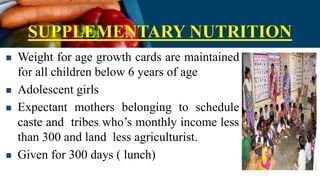
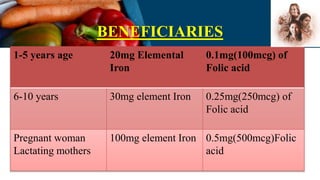
The document outlines the various National Nutritional Programmes in India, focusing on child health and nursing. It details the objectives, policies, and specific programmes initiated by different ministries aimed at improving the nutritional status of children and addressing malnutrition. Key initiatives include the Integrated Child Development Services (ICDS), Mid-Day Meal Programme, and Nutrition Programmes for pregnant, lactating women, and adolescent girls, which aim to enhance health outcomes and reduce malnutrition in vulnerable populations.