Downloaded 225 times

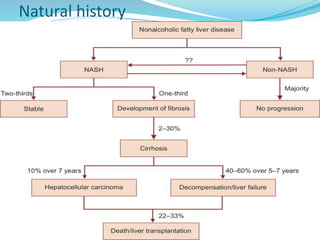
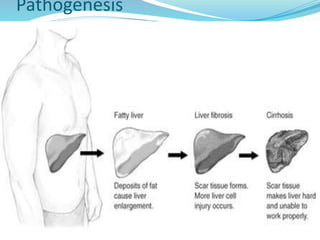
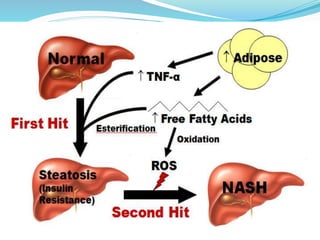
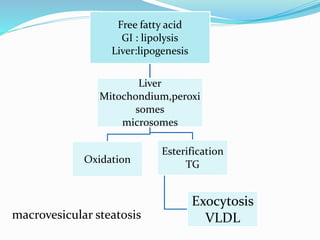
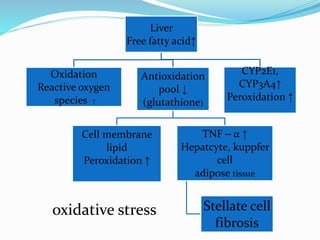
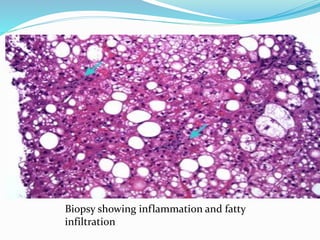




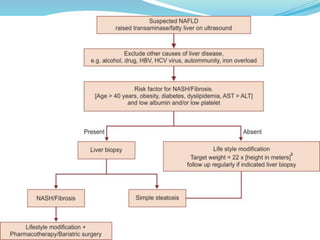


Non-alcoholic fatty liver disease (NAFLD) encompasses a spectrum from simple fatty liver to non-alcoholic steatohepatitis (NASH), with significant global prevalence, particularly among obese and diabetic patients. The pathogenesis involves a two-hit hypothesis leading to liver inflammation and possible progression to cirrhosis, while diagnostic approaches include imaging and liver biopsy to assess liver damage. Treatment focuses on managing associated risk factors, lifestyle changes, and, in some cases, pharmacological interventions, with ongoing monitoring for complications such as hepatocellular carcinoma in advanced cases.












































































