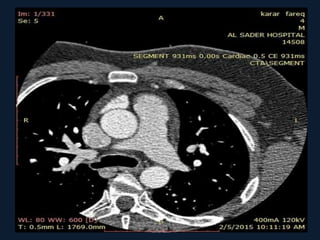
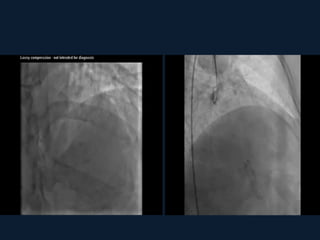
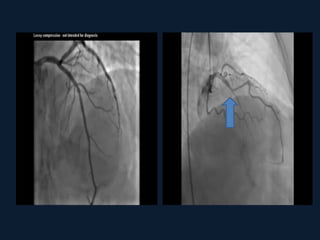
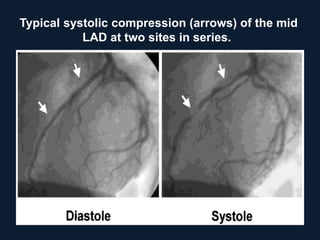
A 27-year old male presented with chest pain and was found to have a myocardial bridge after a CT angiogram (CTA). A myocardial bridge is an abnormality where a segment of a coronary artery passes through heart muscle instead of over it. For most patients, a myocardial bridge does not cause problems. However, in some cases it can lead to decreased blood flow and oxygen to the heart muscle (ischemia). The diagnosis is typically made using CTA, angiography, intravascular ultrasound (IVUS), or cardiac MRI. Treatment involves medications if symptoms occur, and rarely surgery is needed to relieve severe angina.