Downloaded 20 times


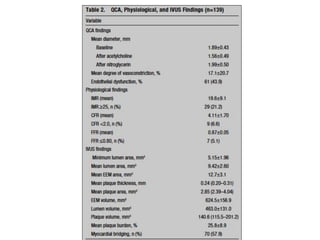
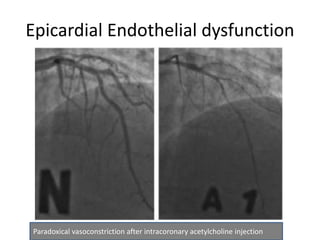
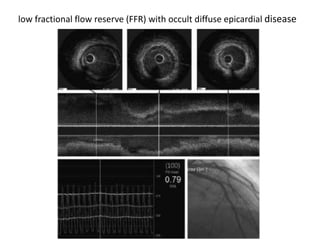
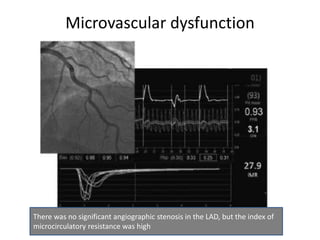
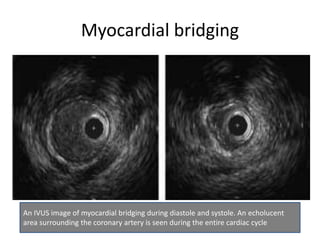
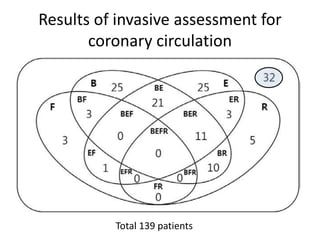
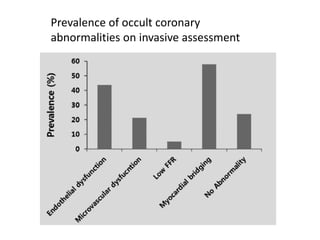
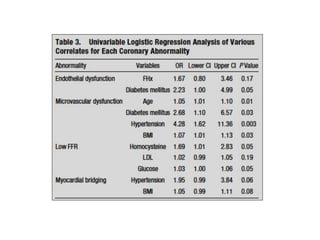
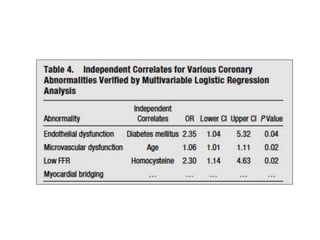
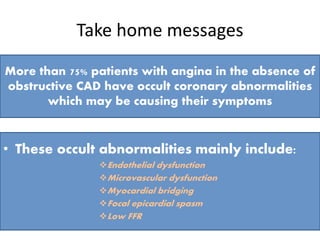

This study investigated the potential underlying causes of angina in symptomatic patients without obstructive coronary artery disease (CAD) using a comprehensive combination of invasive investigations. The study found that more than 75% of patients had occult coronary abnormalities, including endothelial dysfunction, microvascular dysfunction, myocardial bridging, focal epicardial spasm, and low fractional flow reserve values. These findings suggest that invasive assessment can identify abnormal coronary functions that may be causing chest pain in patients whose initial angiograms show nonobstructive CAD. However, the study was limited by its small size and single center design.
















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



