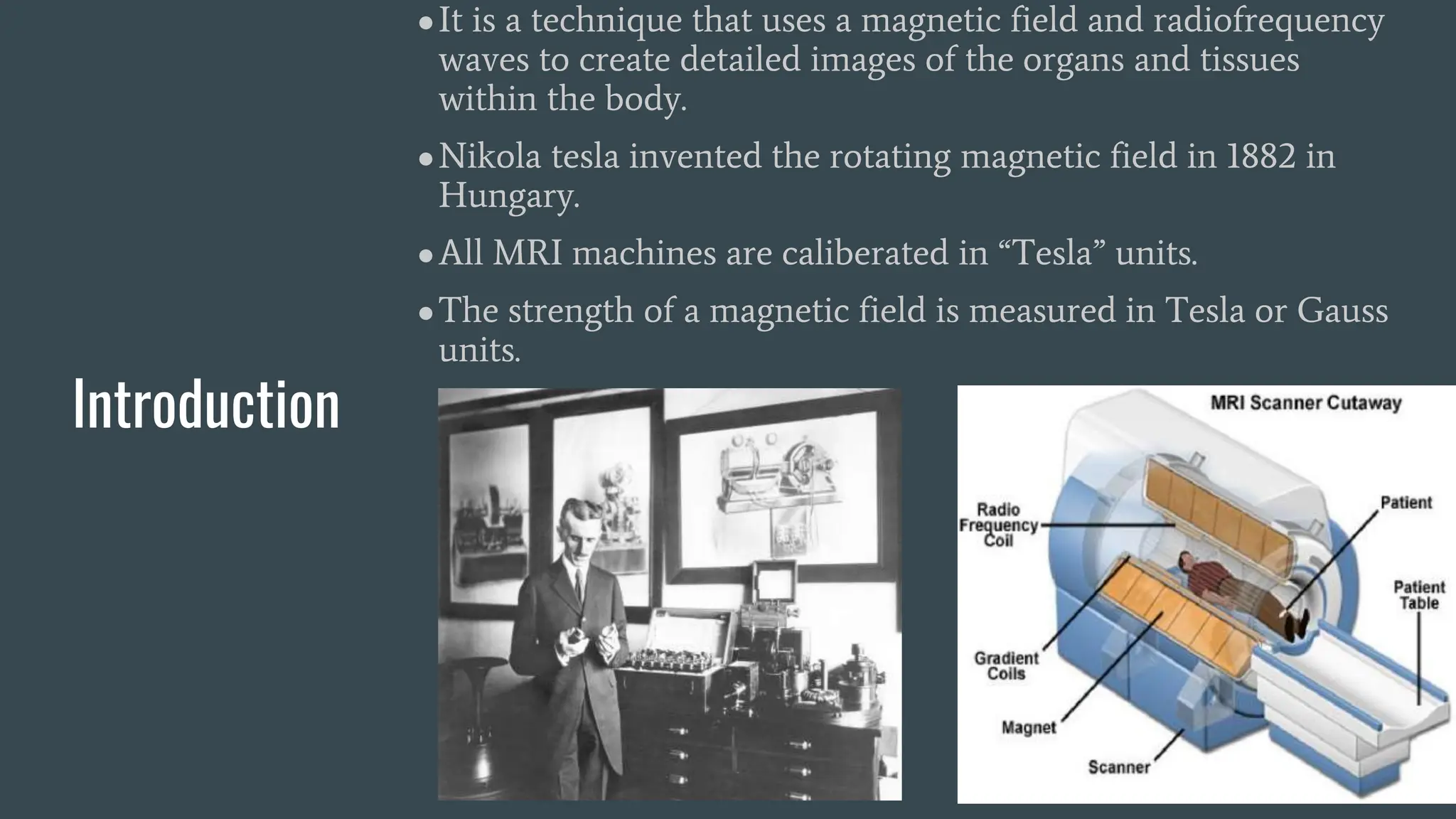
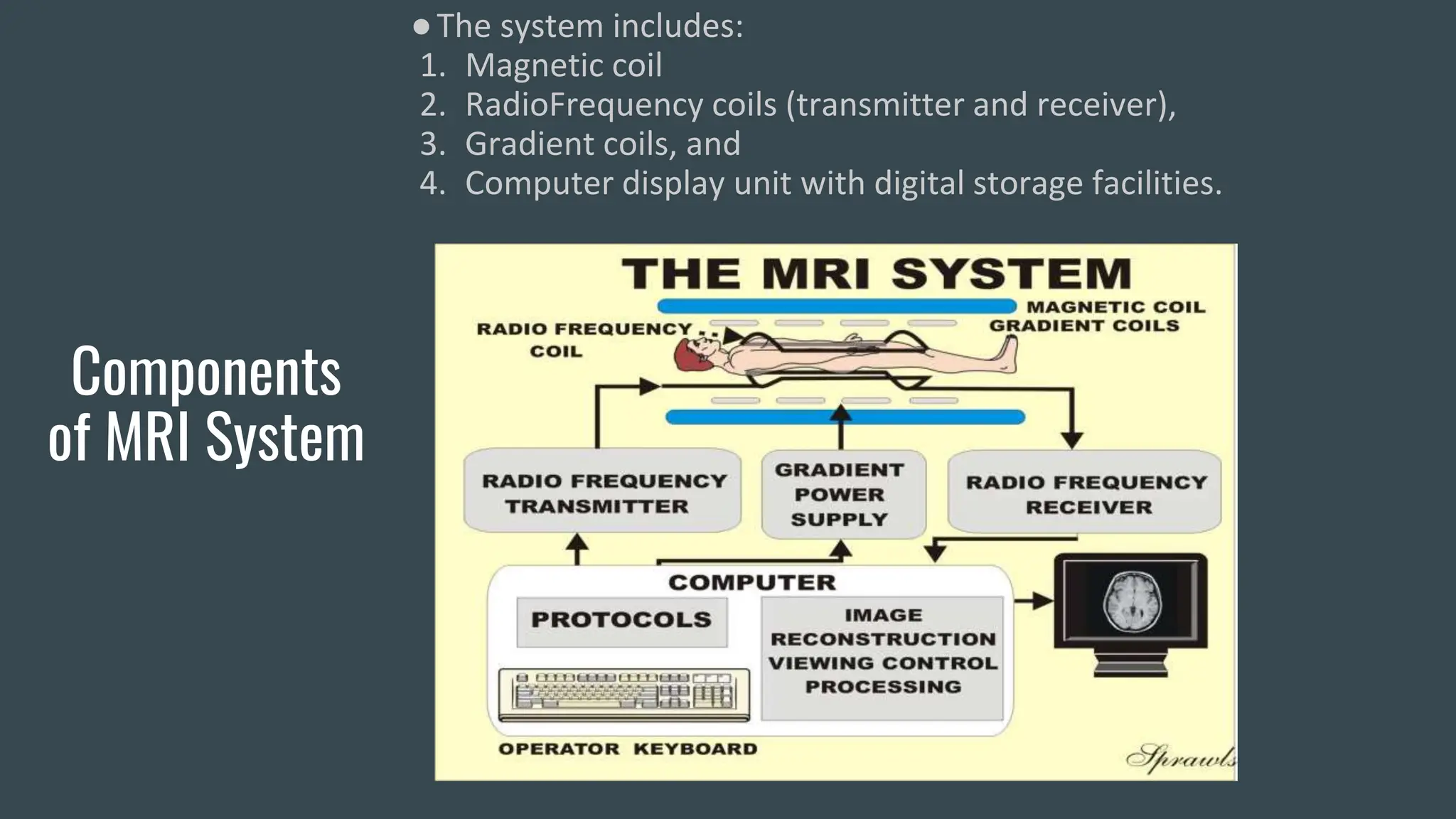
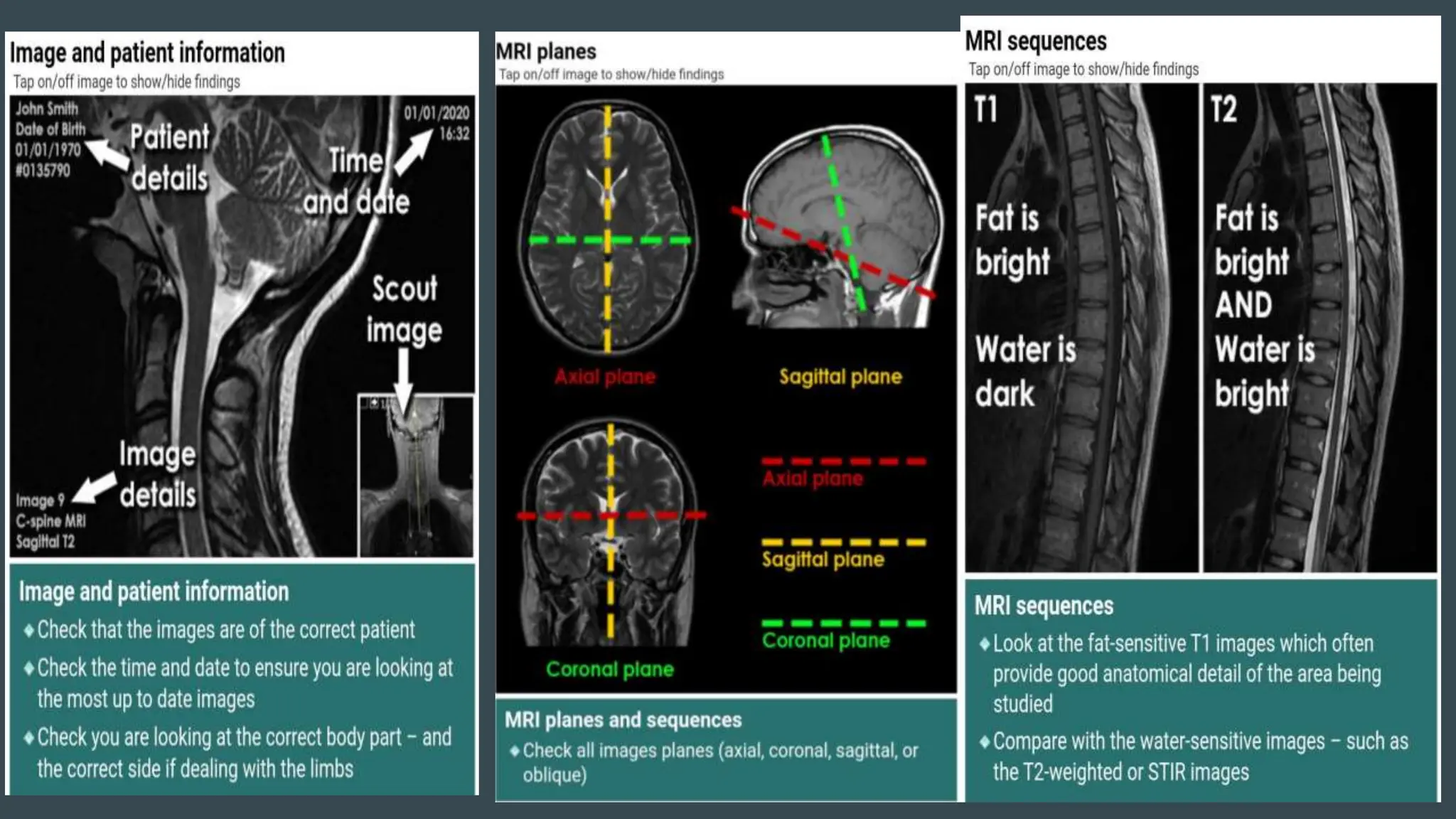
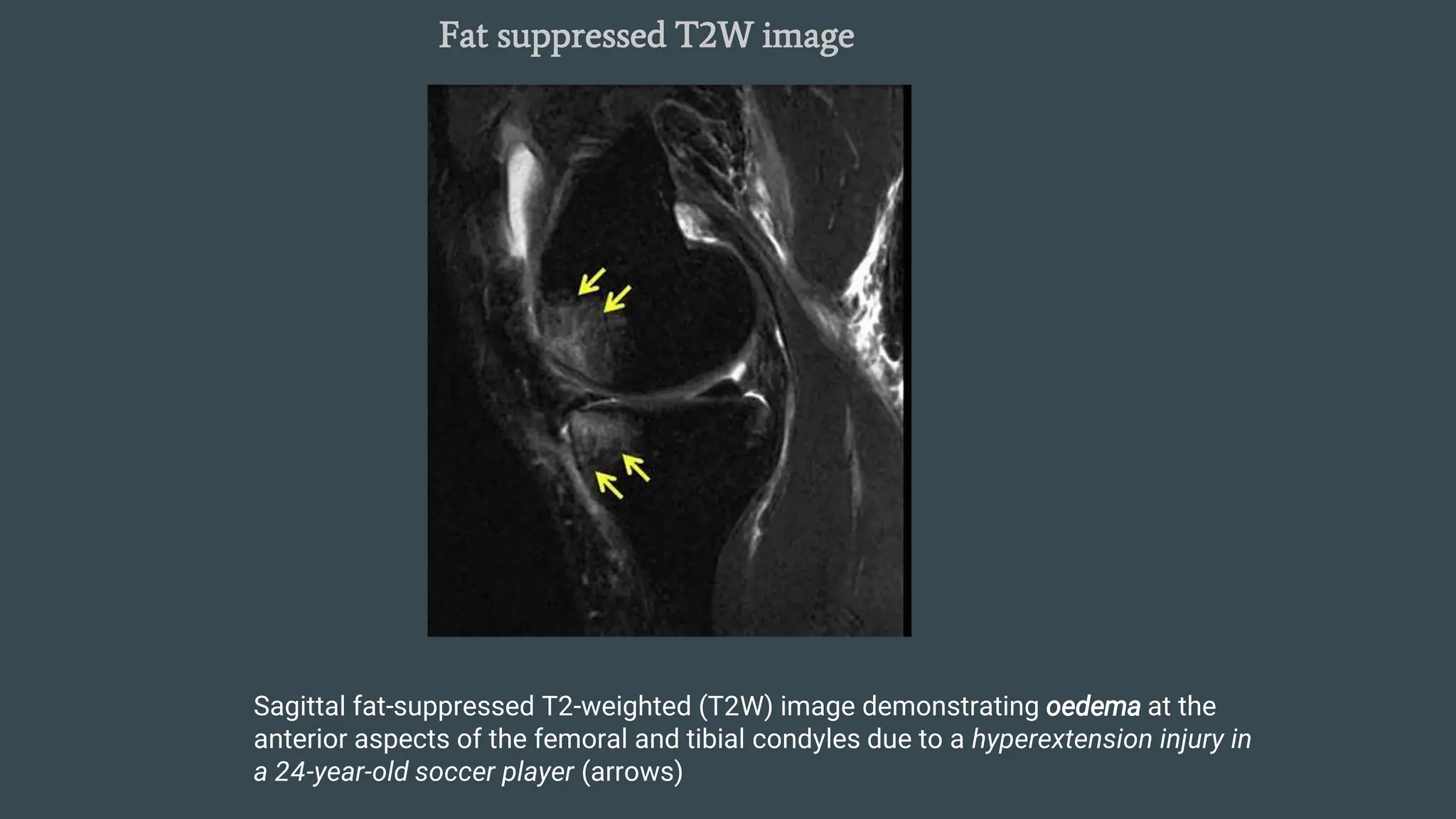
MRI uses magnetic fields and radio waves to produce detailed images of organs and tissues inside the body. An MRI scanner contains magnetic coils, radiofrequency coils, gradient coils, and a computer display unit. MRI works by aligning atomic nuclei such as hydrogen in a magnetic field and inducing resonance with radio pulses. When the pulses are removed, the nuclei release energy that is detected as signals providing data to create digital images. MRI can produce different types of weighted images like T1, T2, STIR, and gradient echo that highlight various tissues. MRI is useful for imaging musculoskeletal injuries, tumors, infections and other orthopedic conditions due to its excellent soft tissue contrast without ionizing radiation.