Download as PDF, PPTX
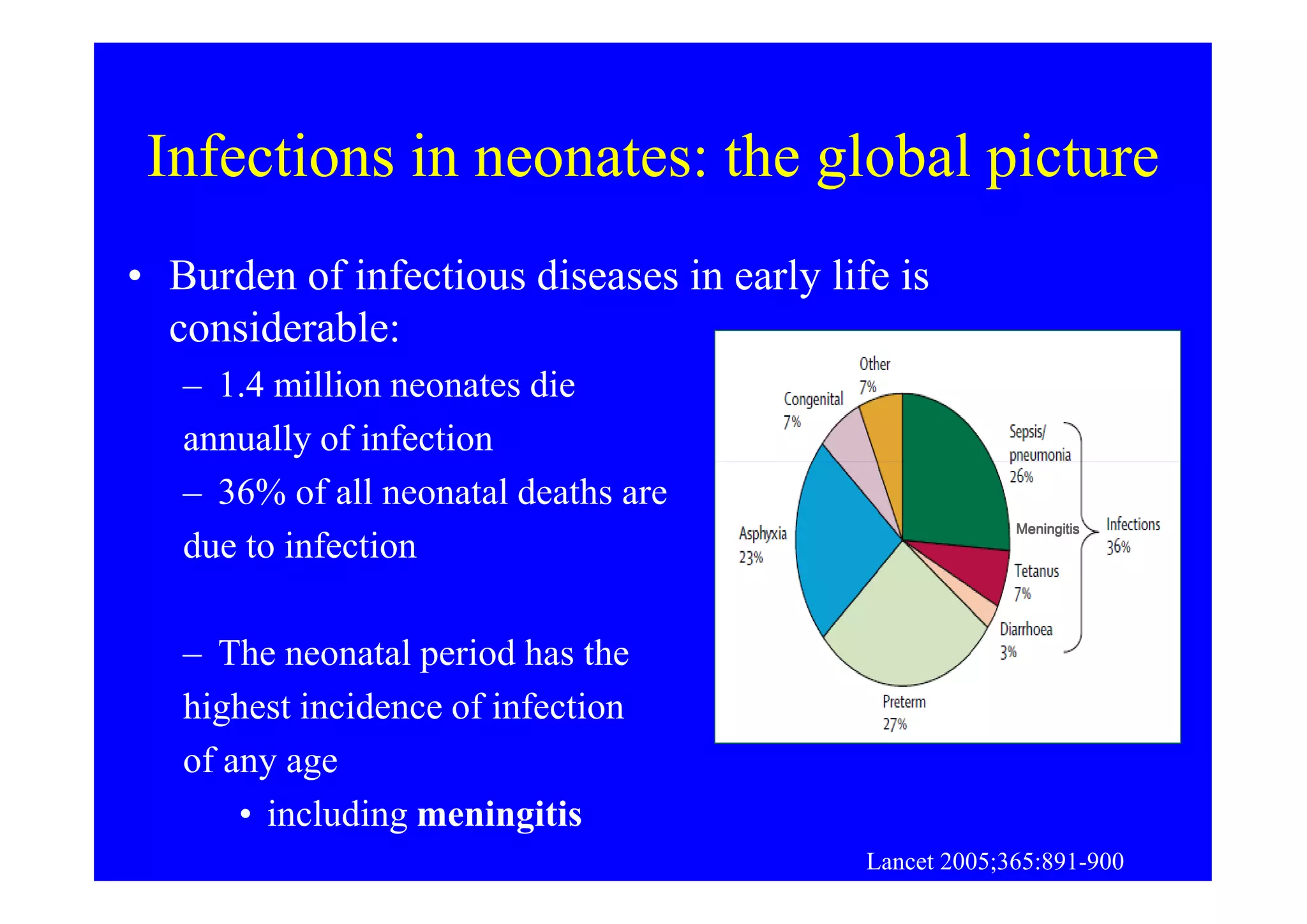
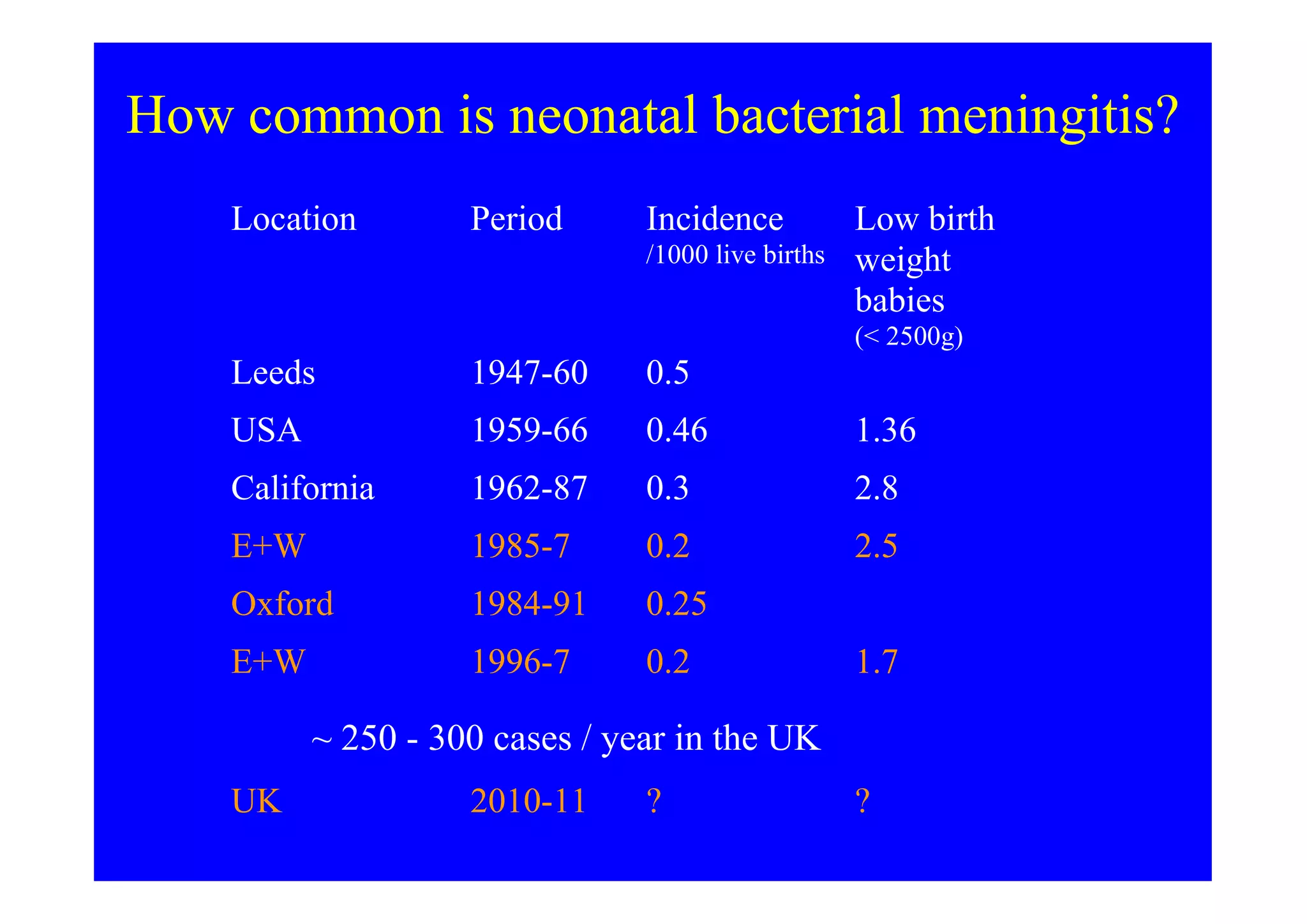
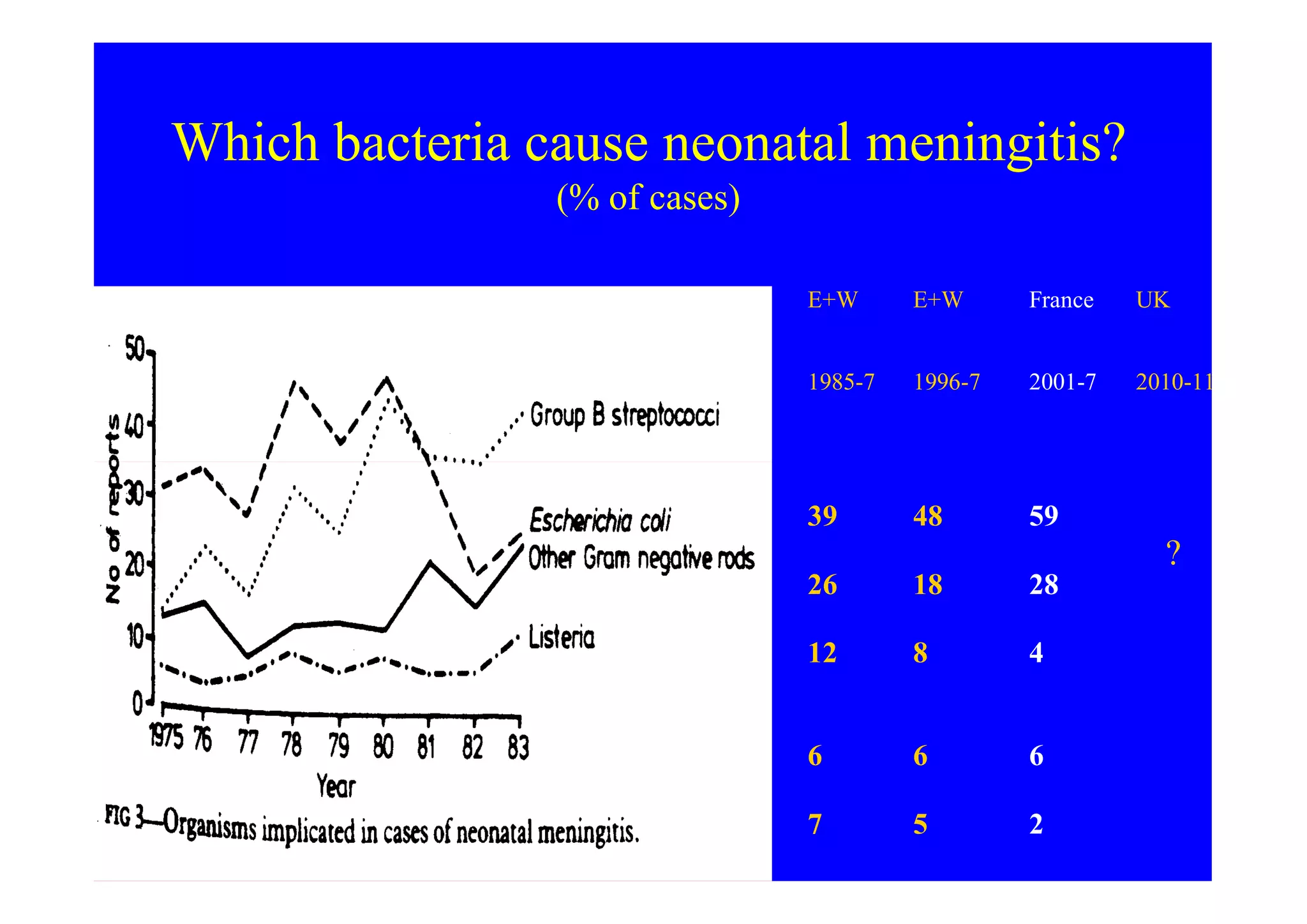
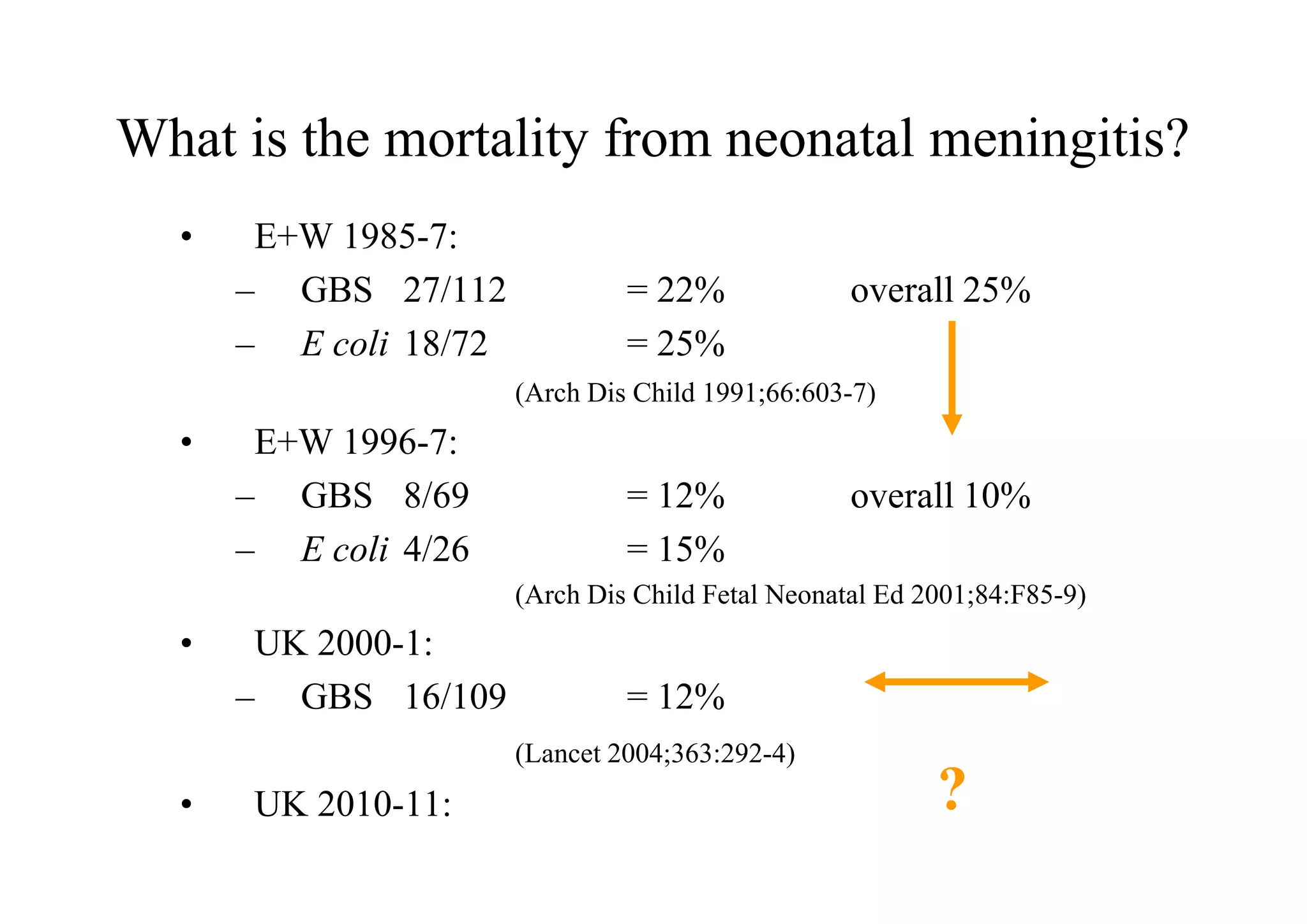
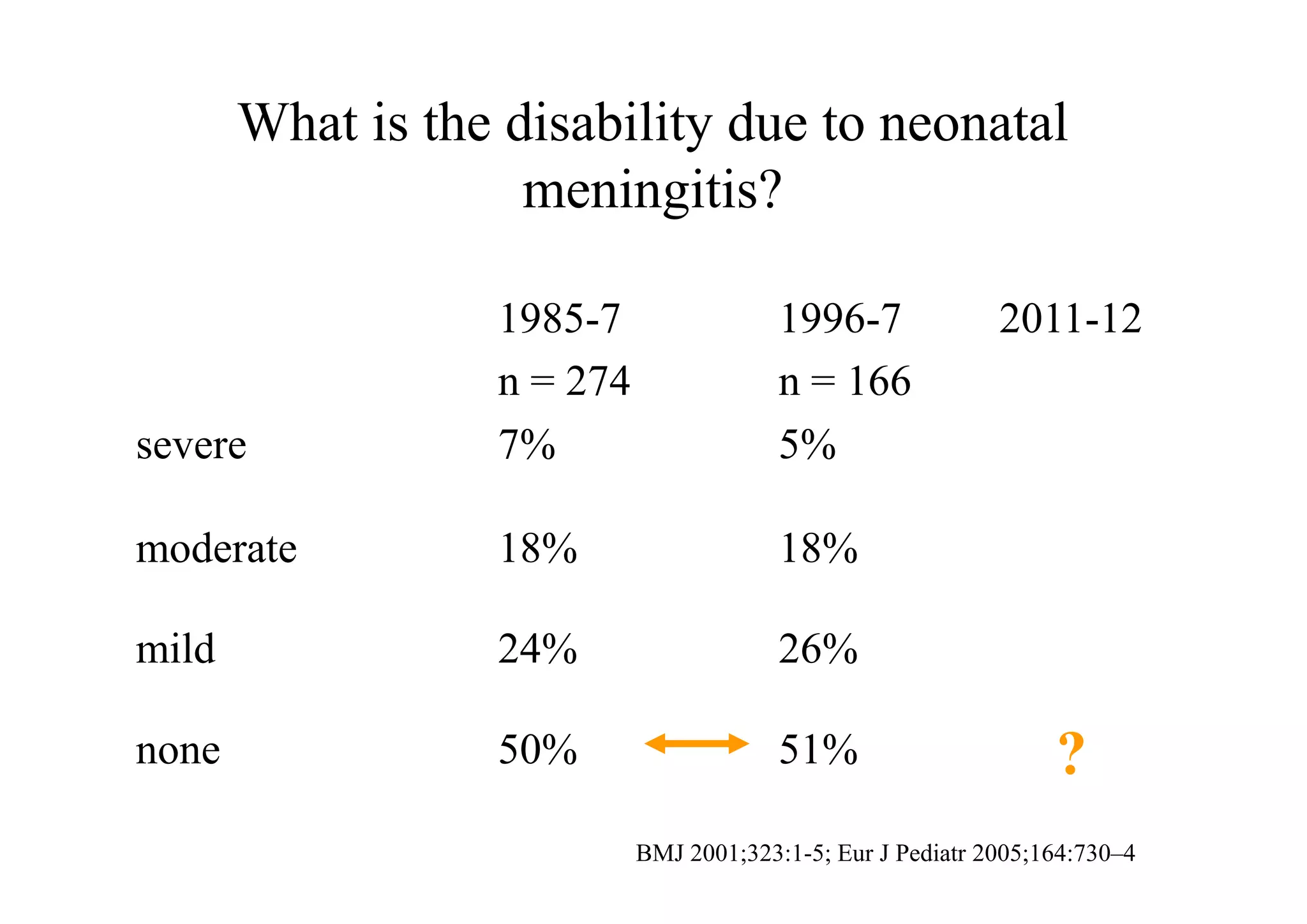
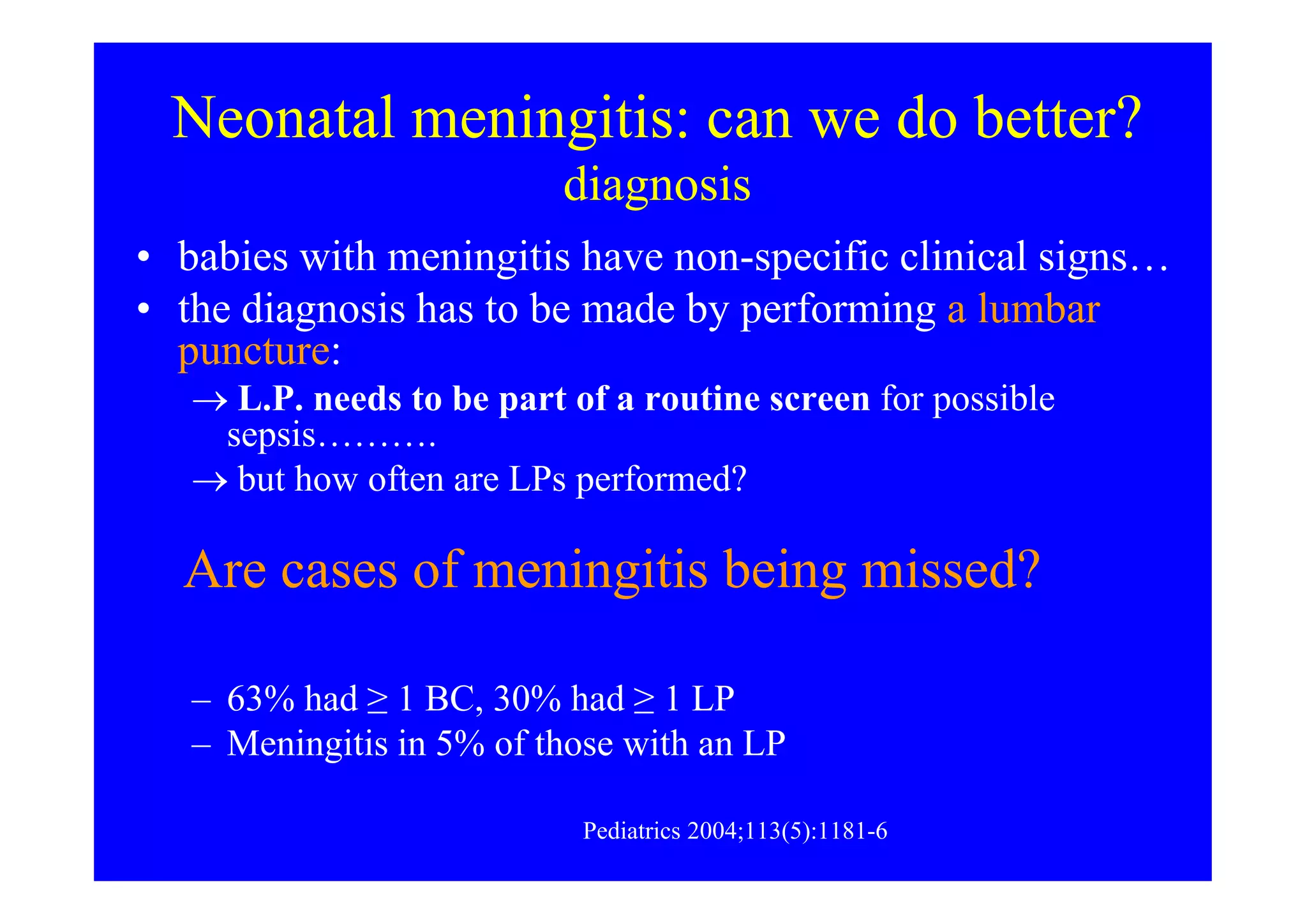
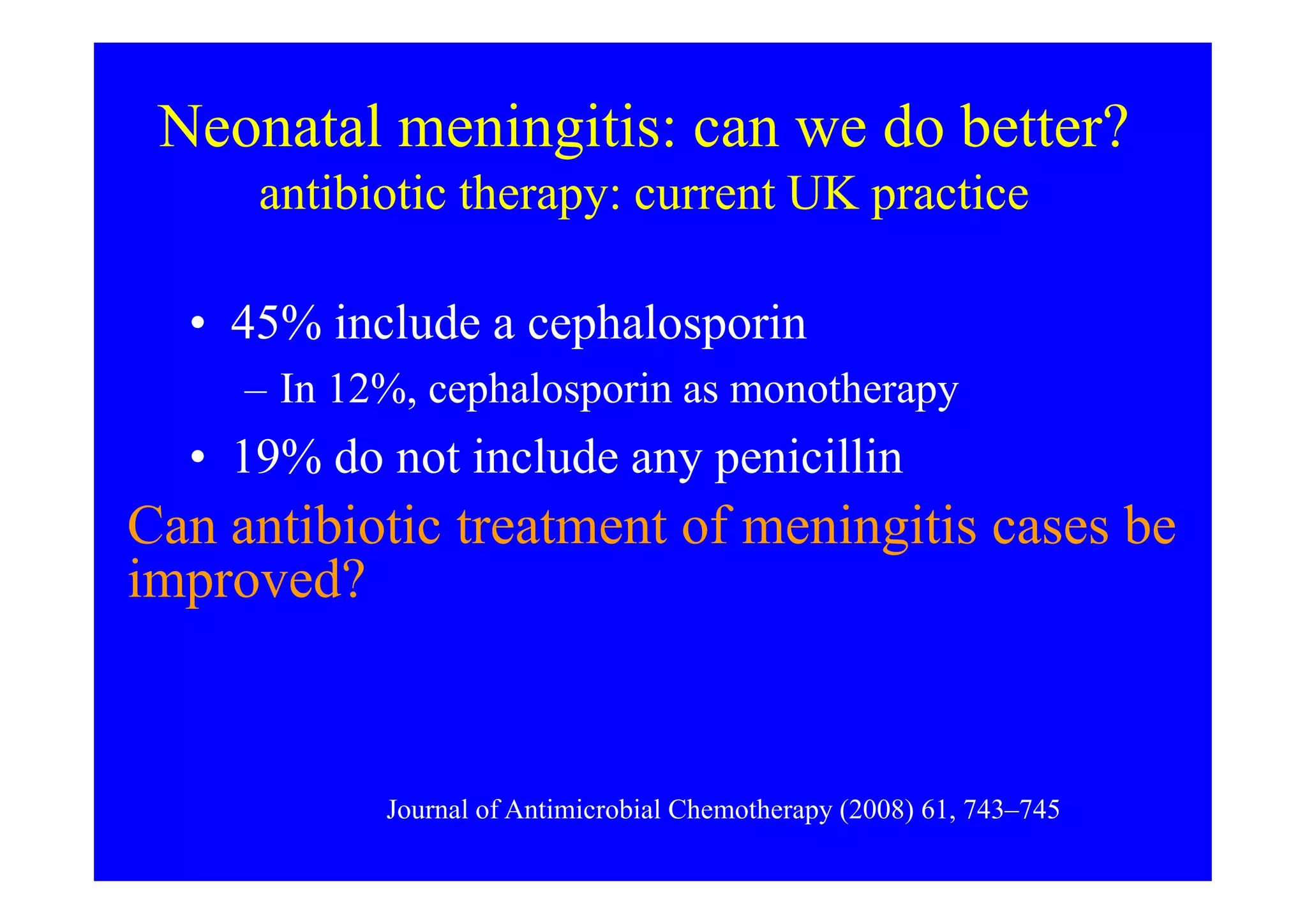
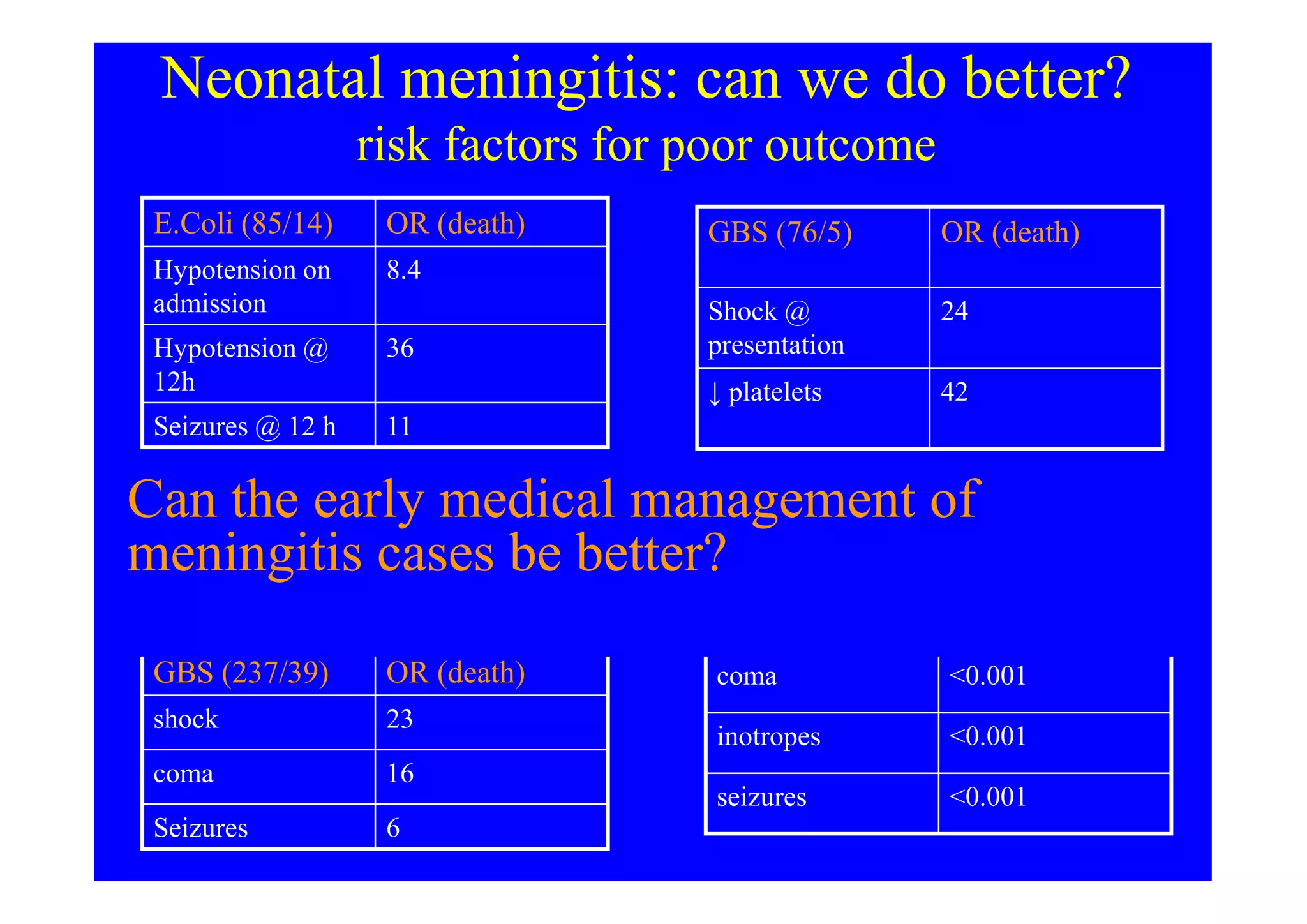

This document discusses neonatal meningitis and outlines opportunities to improve outcomes. It notes that 1) neonatal meningitis is a significant global cause of infant mortality, with Group B Streptococcus and E. coli as leading causes; 2) current UK mortality rates are 10-12% but management may be suboptimal; and 3) a new study aims to define the current burden of neonatal meningitis and identify ways to improve outcomes through earlier diagnosis, optimal antibiotic use, and supportive care.









































![MENINGITIS[1].pdf in pediatric and child health](https://cdn.slidesharecdn.com/ss_thumbnails/meningitis1-250427211208-24875610-thumbnail.jpg?width=640&height=640&fit=bounds)





































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)







