Downloaded 21 times






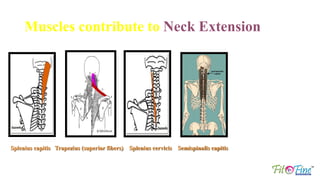
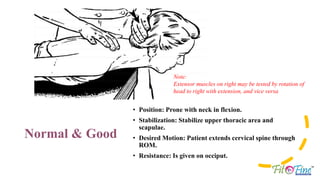
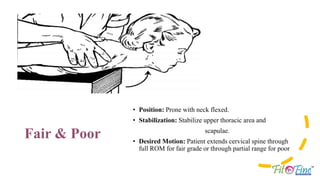


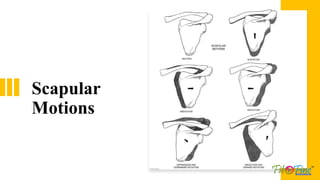
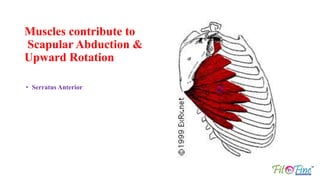

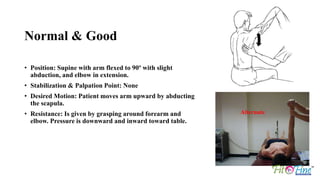

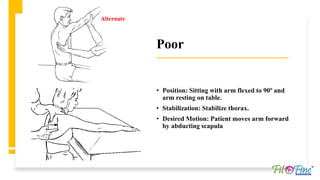













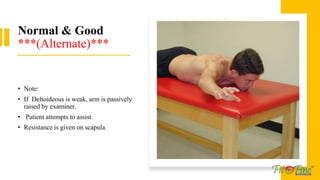
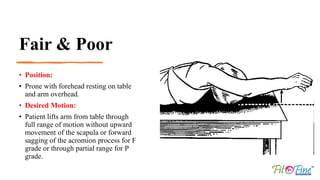
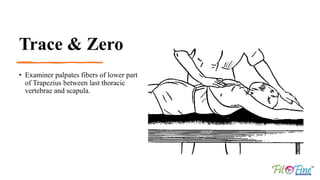










The document outlines muscle testing procedures for the neck and scapula, detailing the origins, insertions, nerve supply, and factors limiting motion for various muscles involved in these areas. It describes positions and stabilization techniques for accurate testing of muscle strength, while providing criteria for normal to zero muscle function. The testing methods focus on flexion, extension, abduction, elevation, and adduction of the cervical spine and scapula, with specific attention to muscle palpation and resistance application.






















































































