Downloaded 31 times
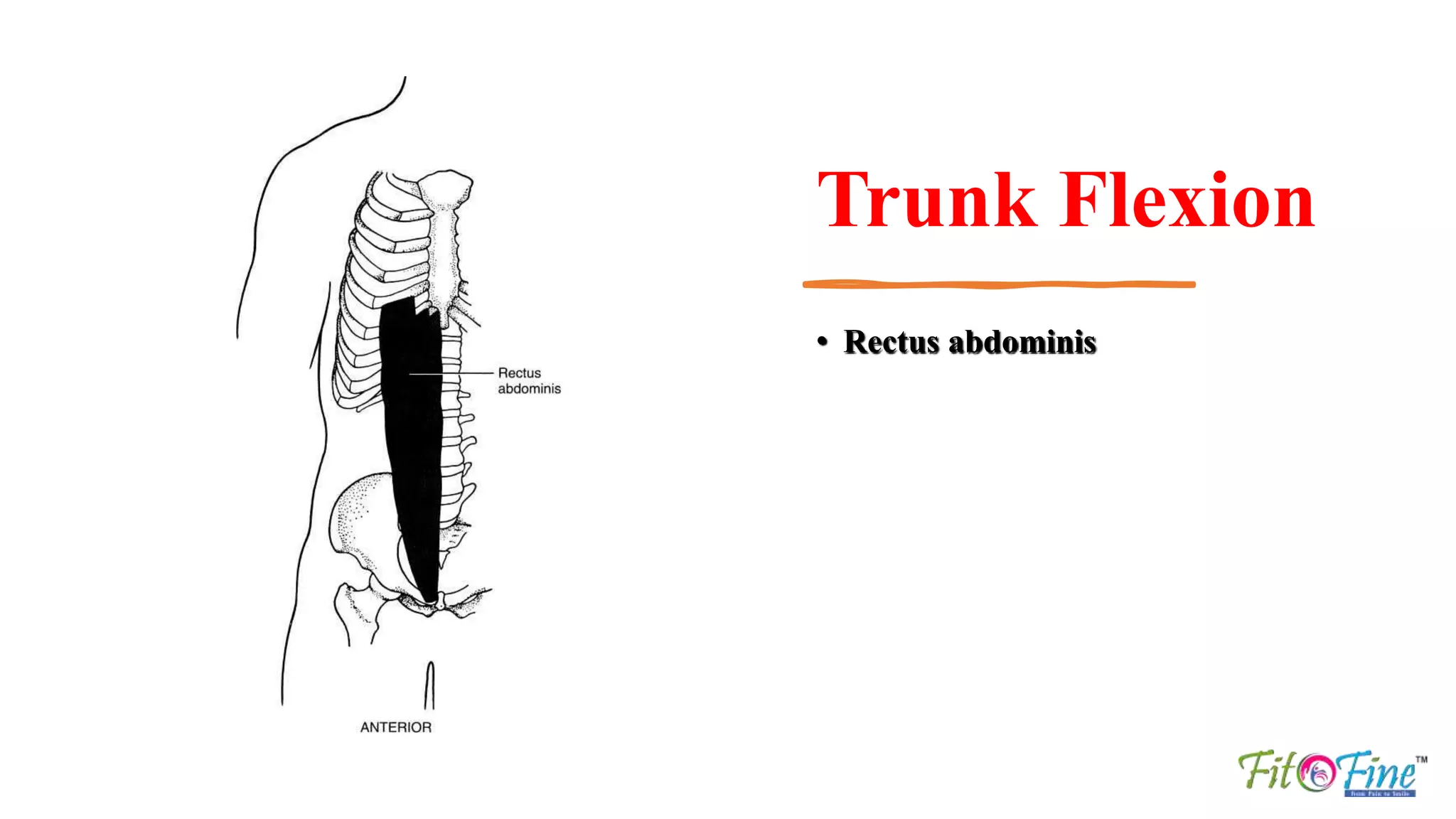
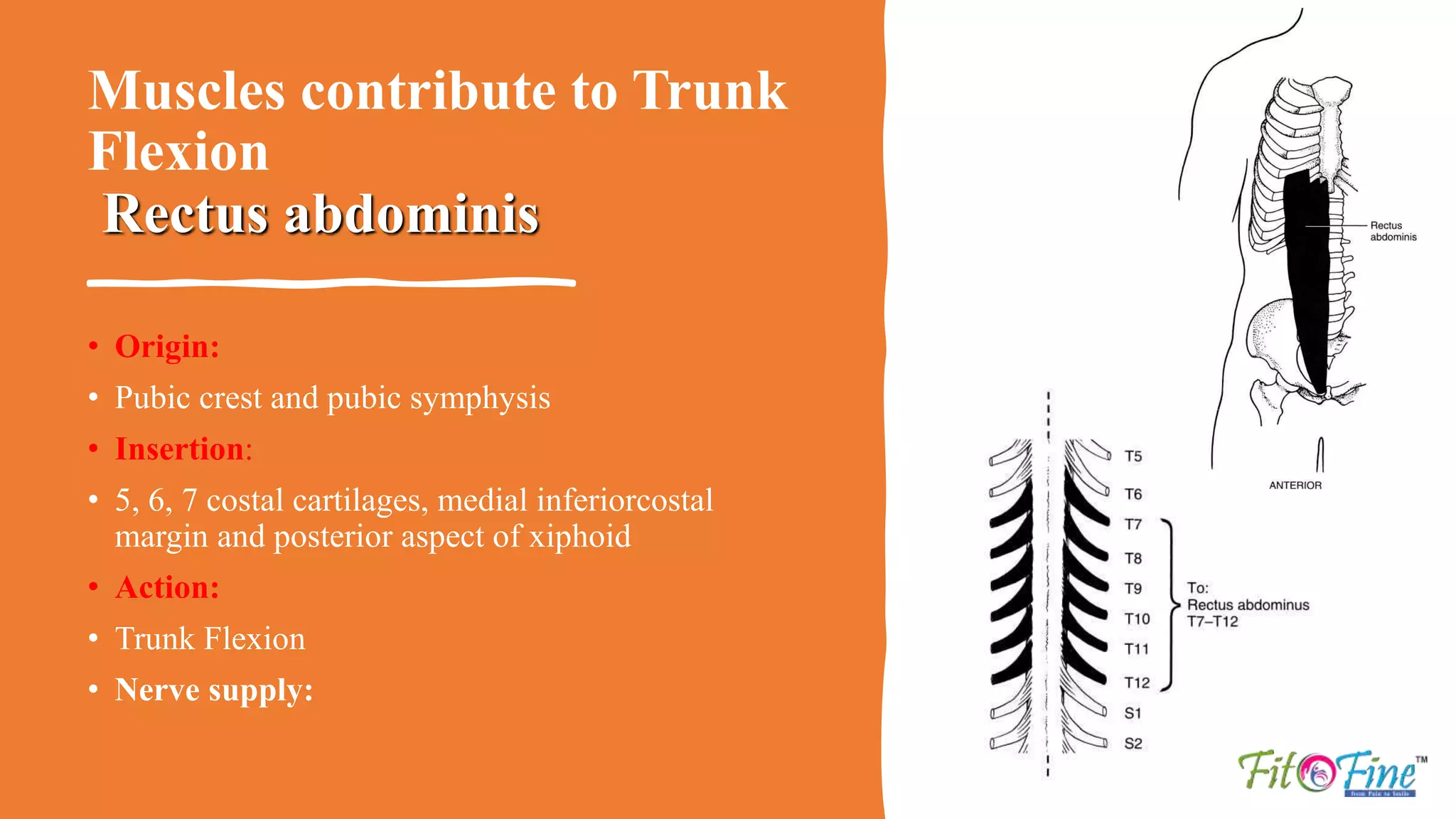
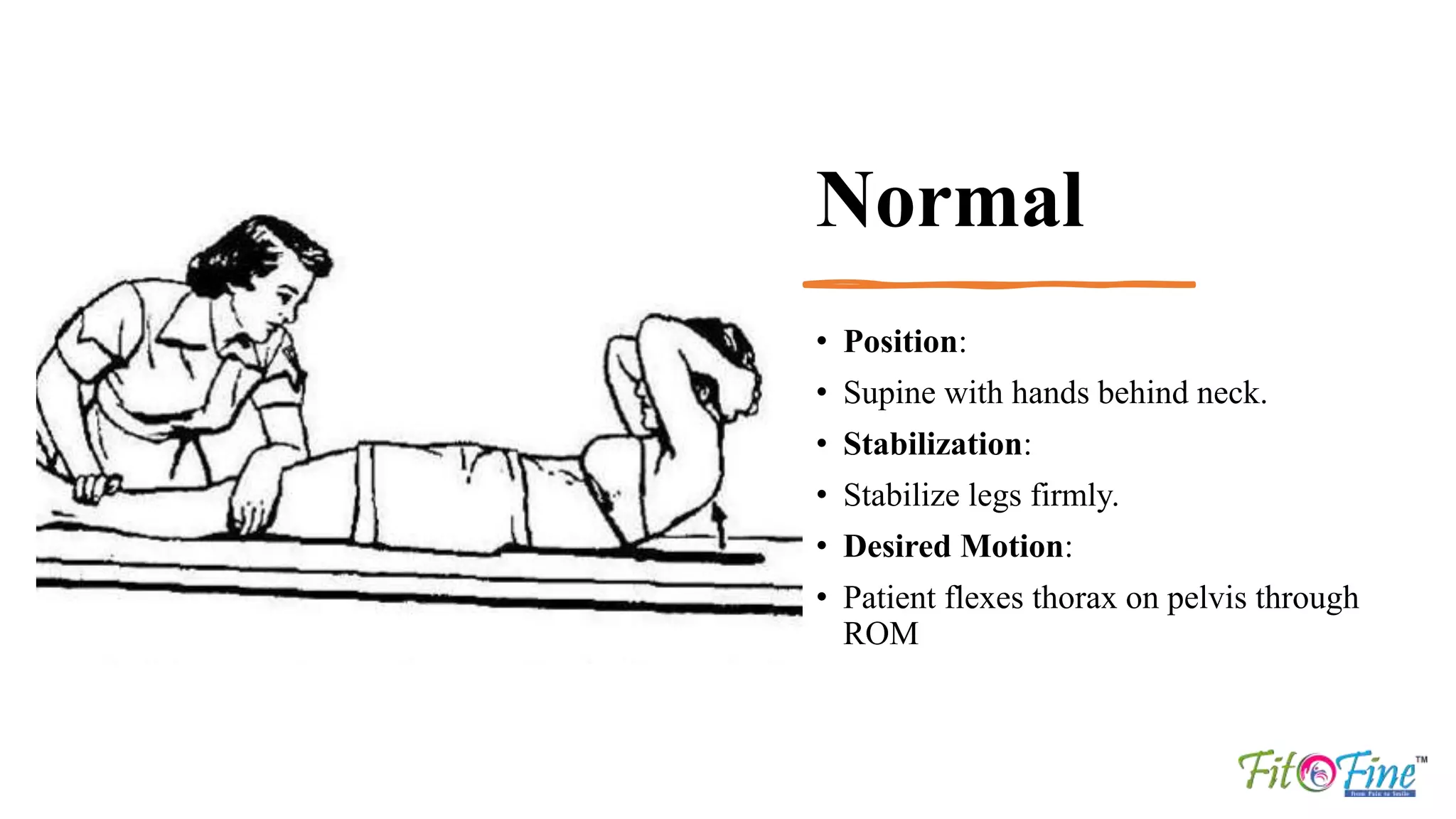
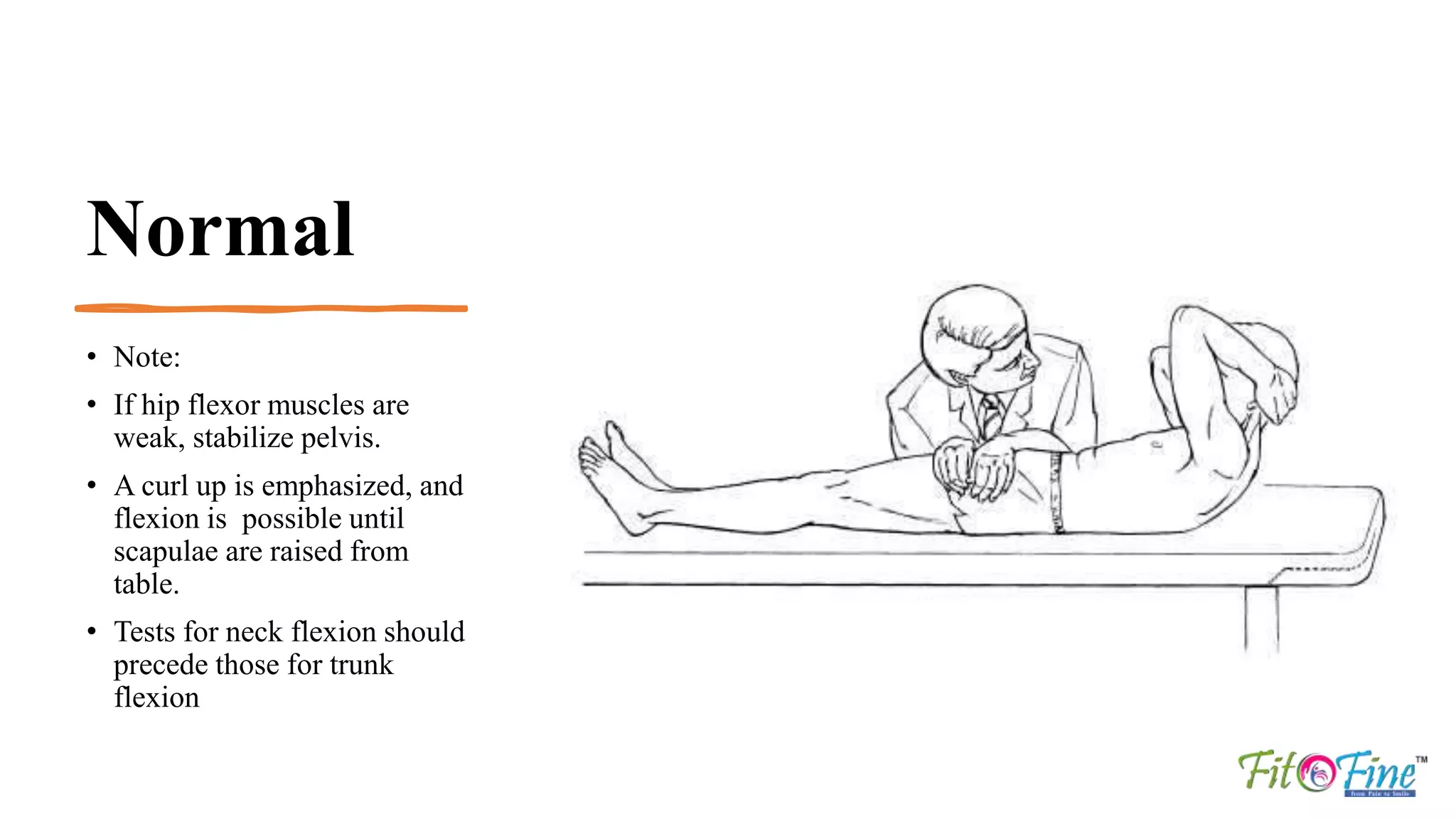
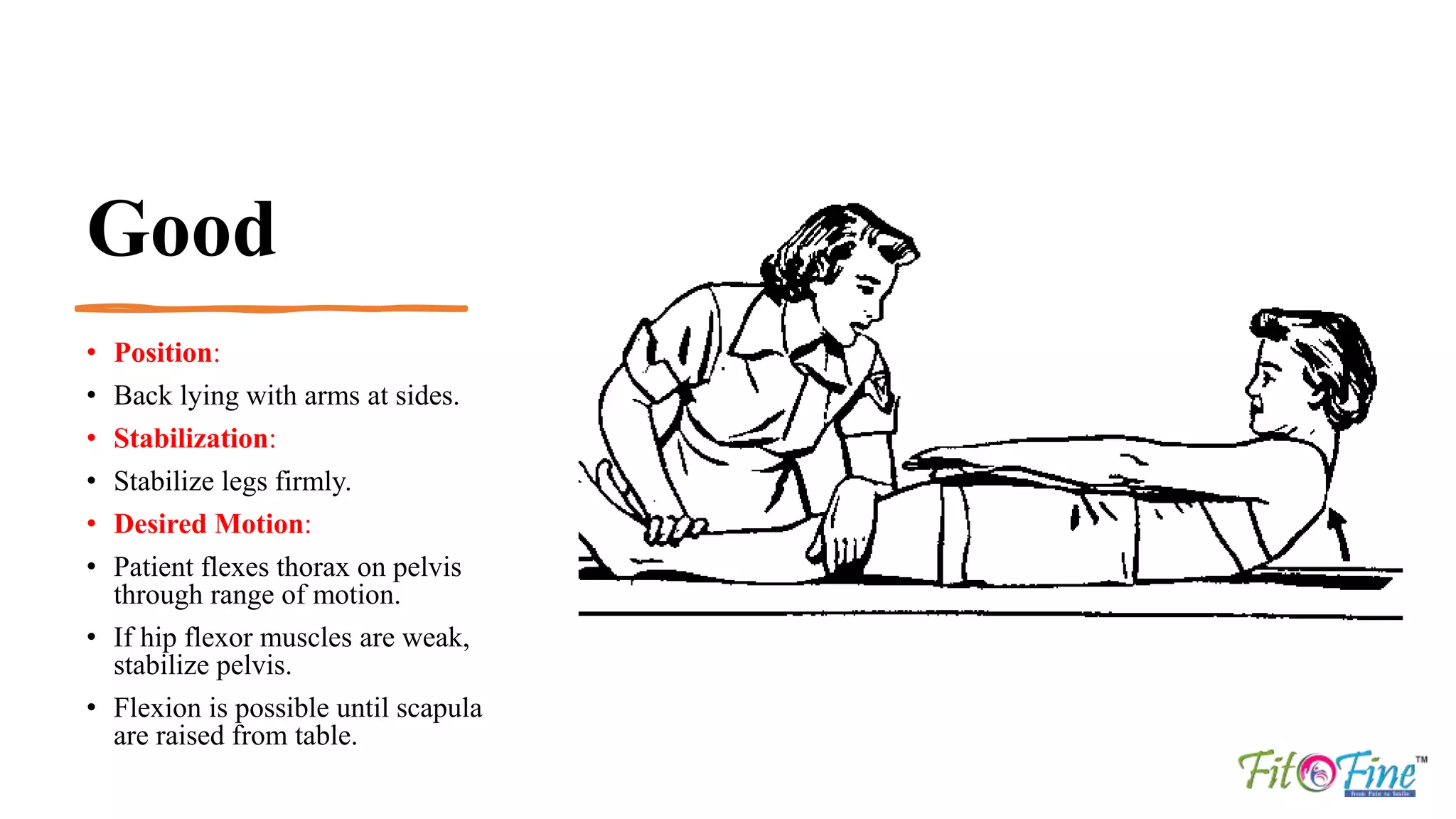
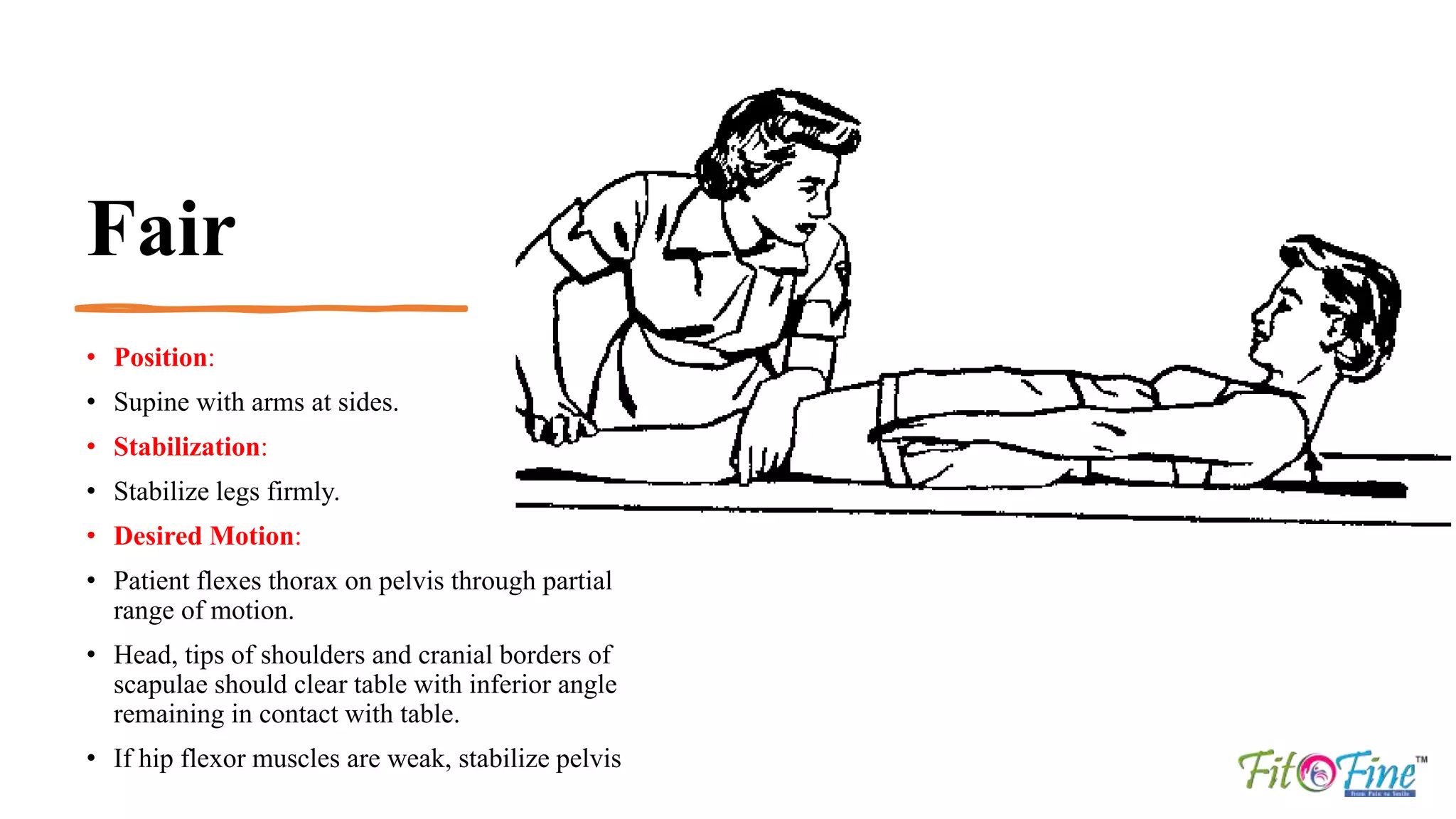
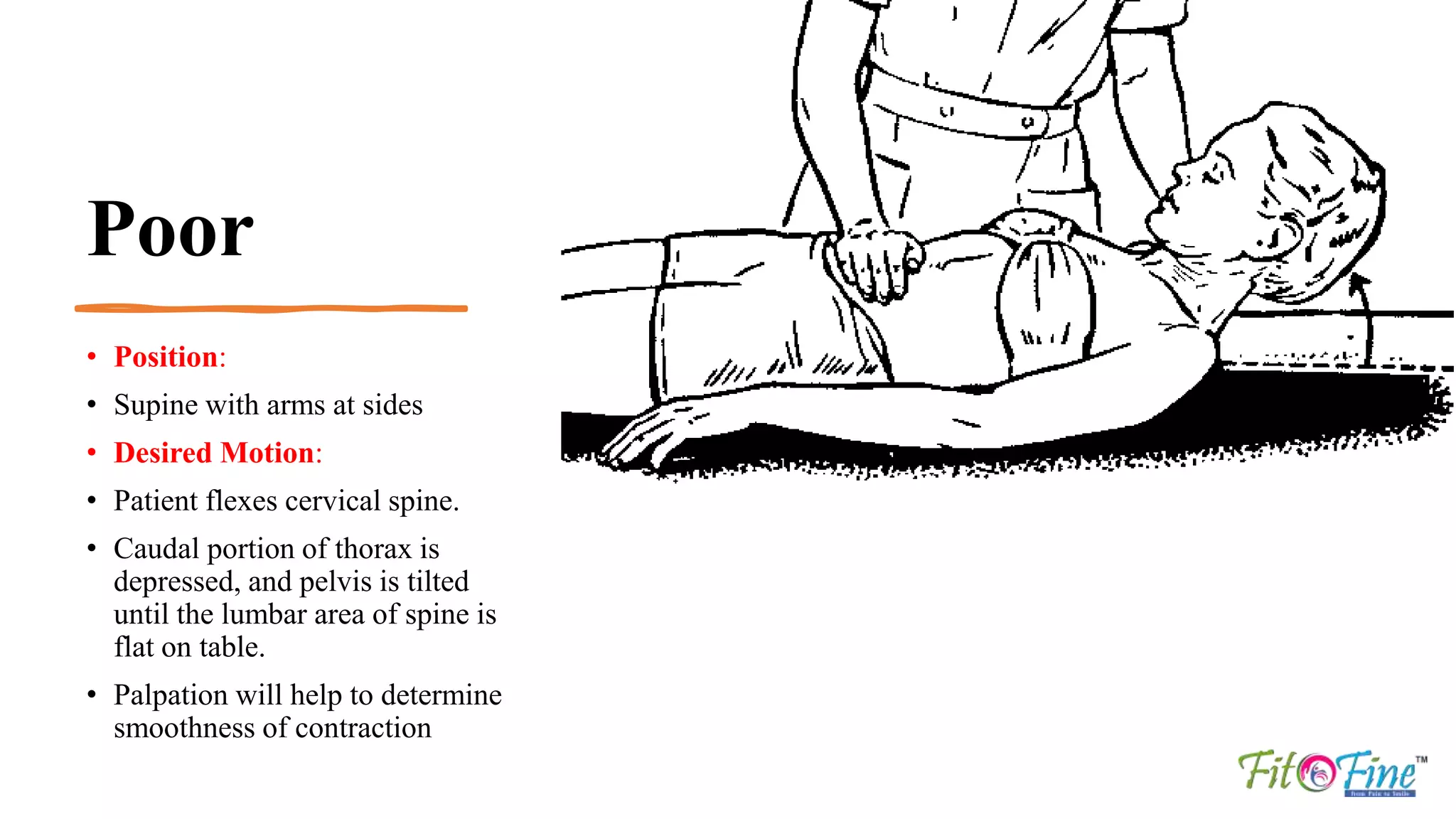
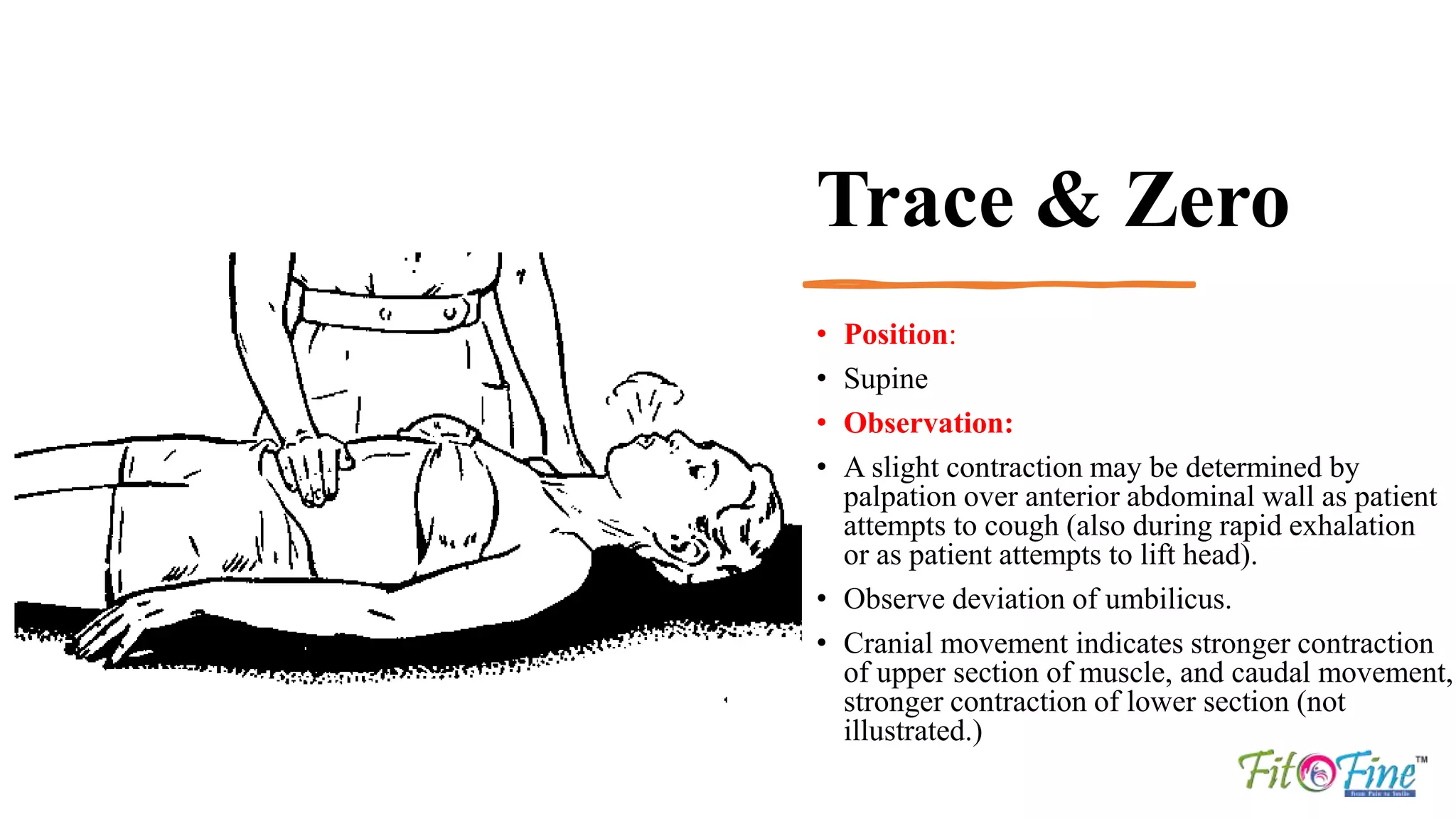
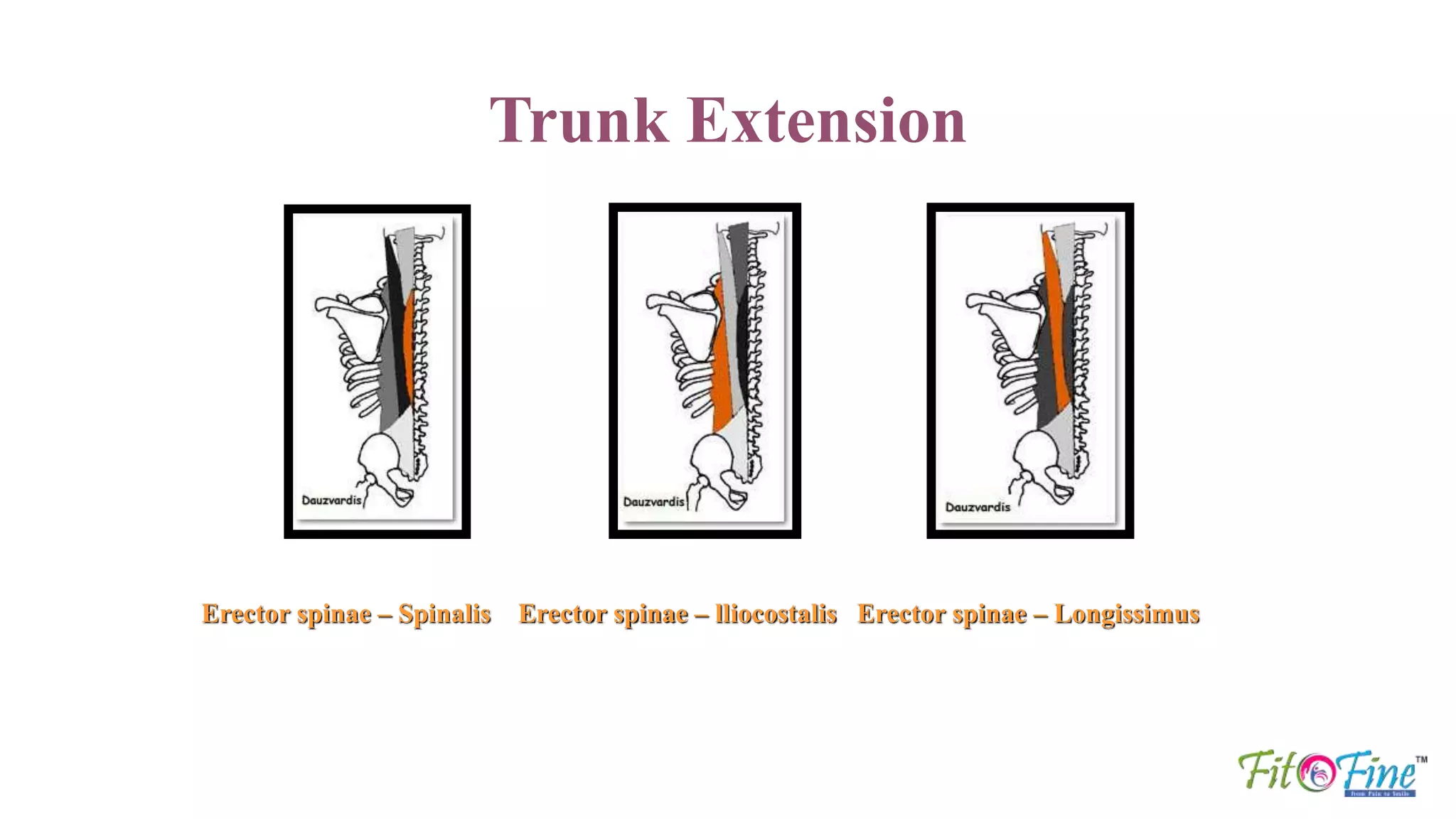
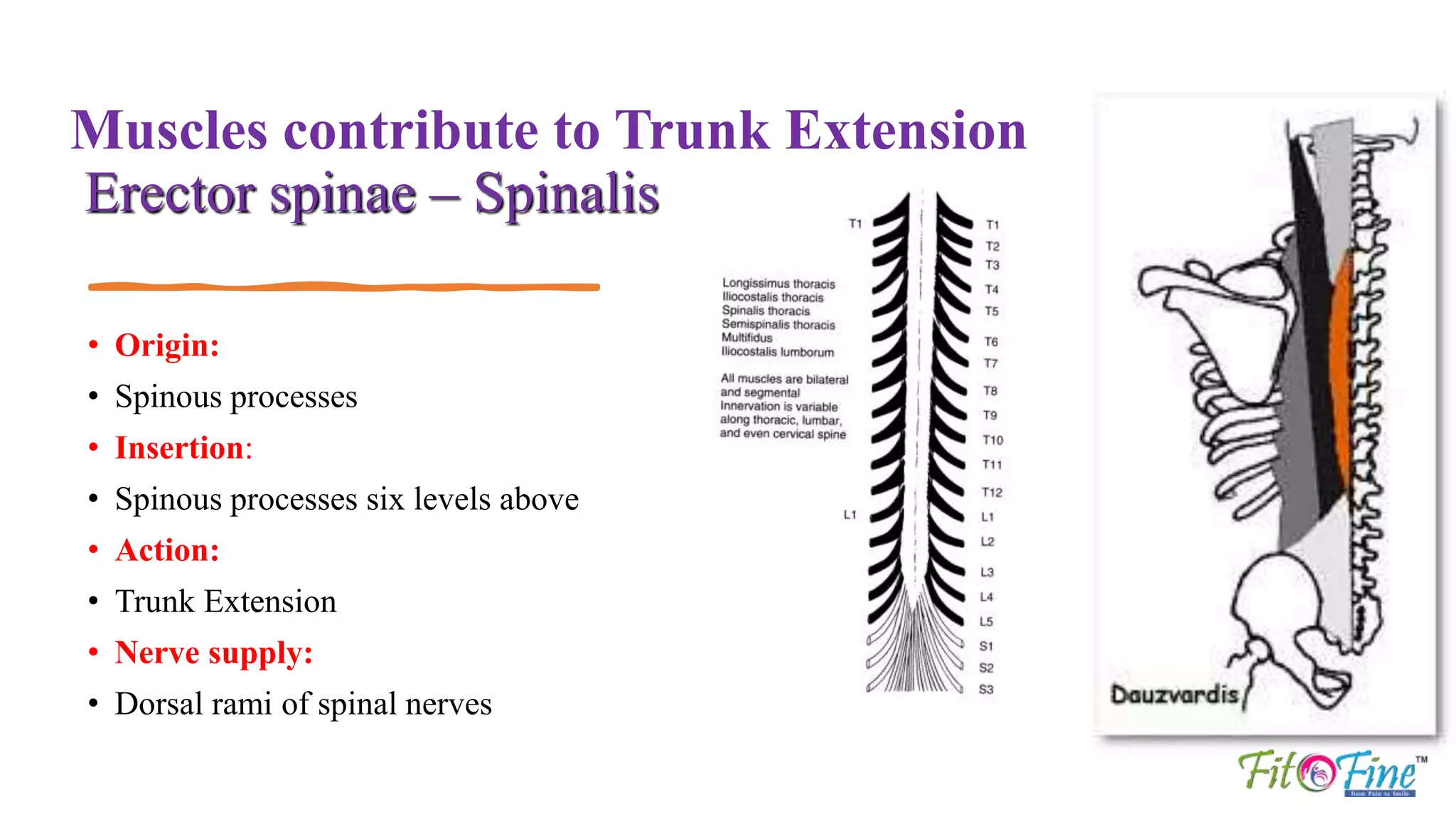
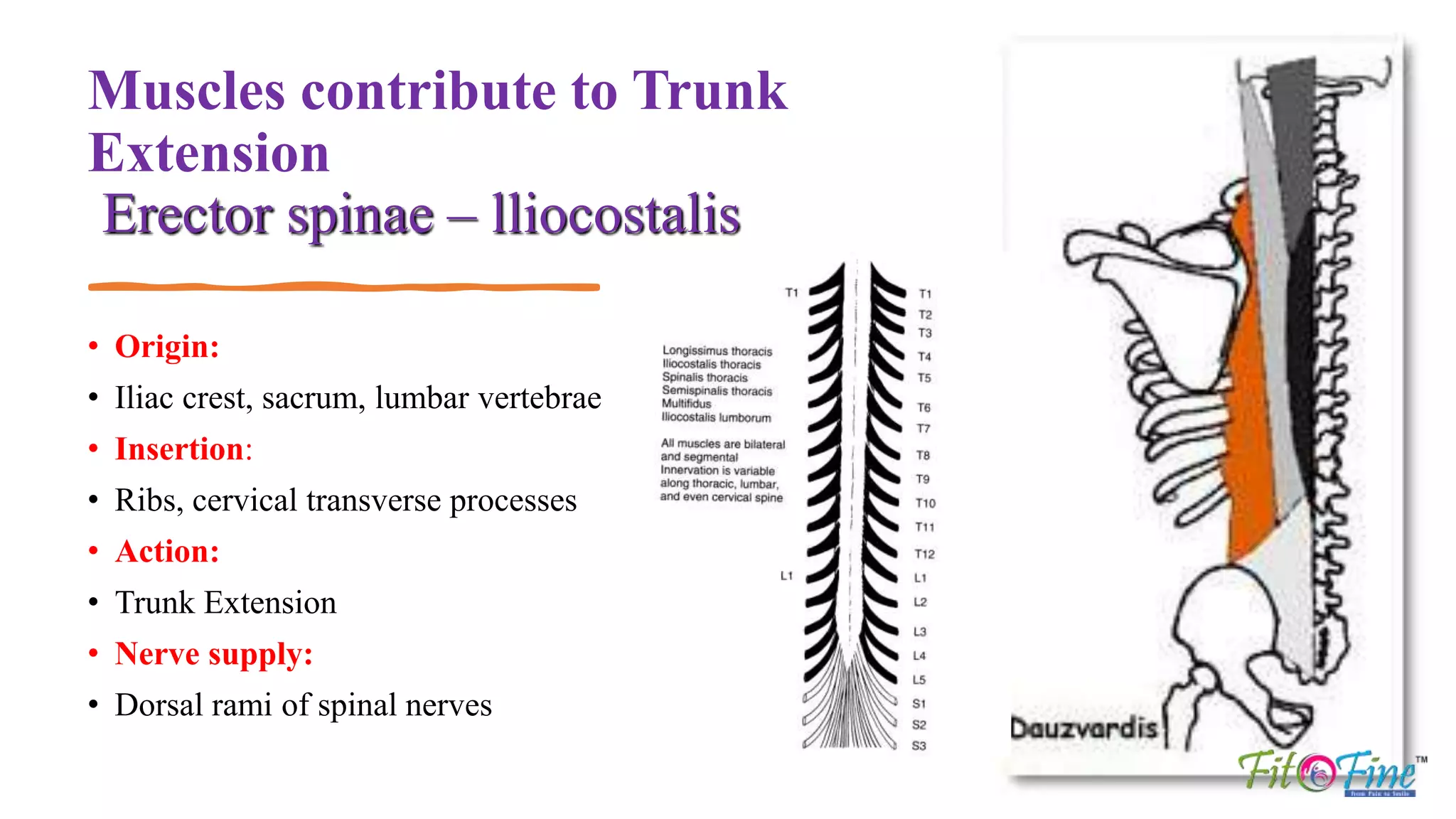
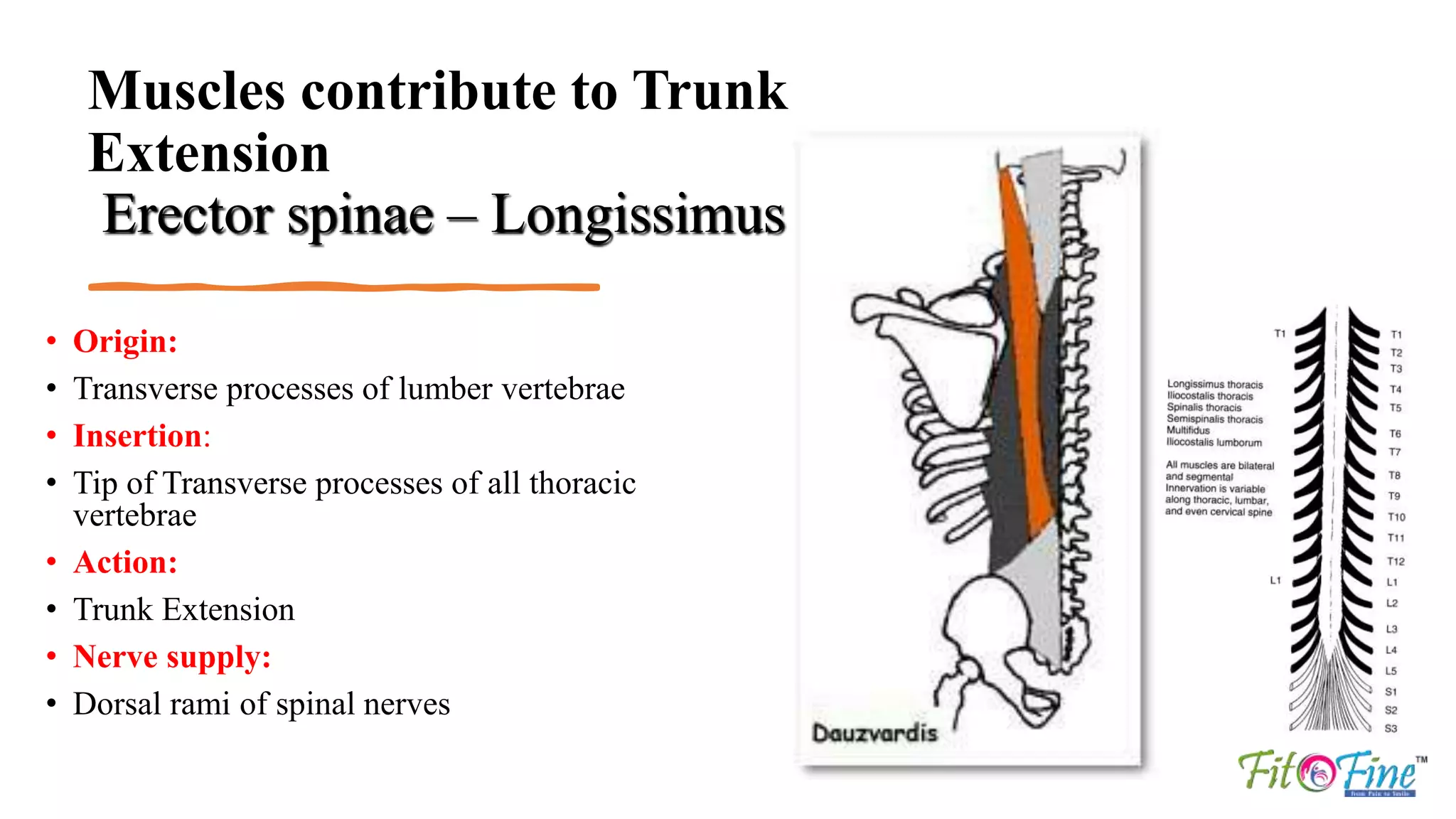

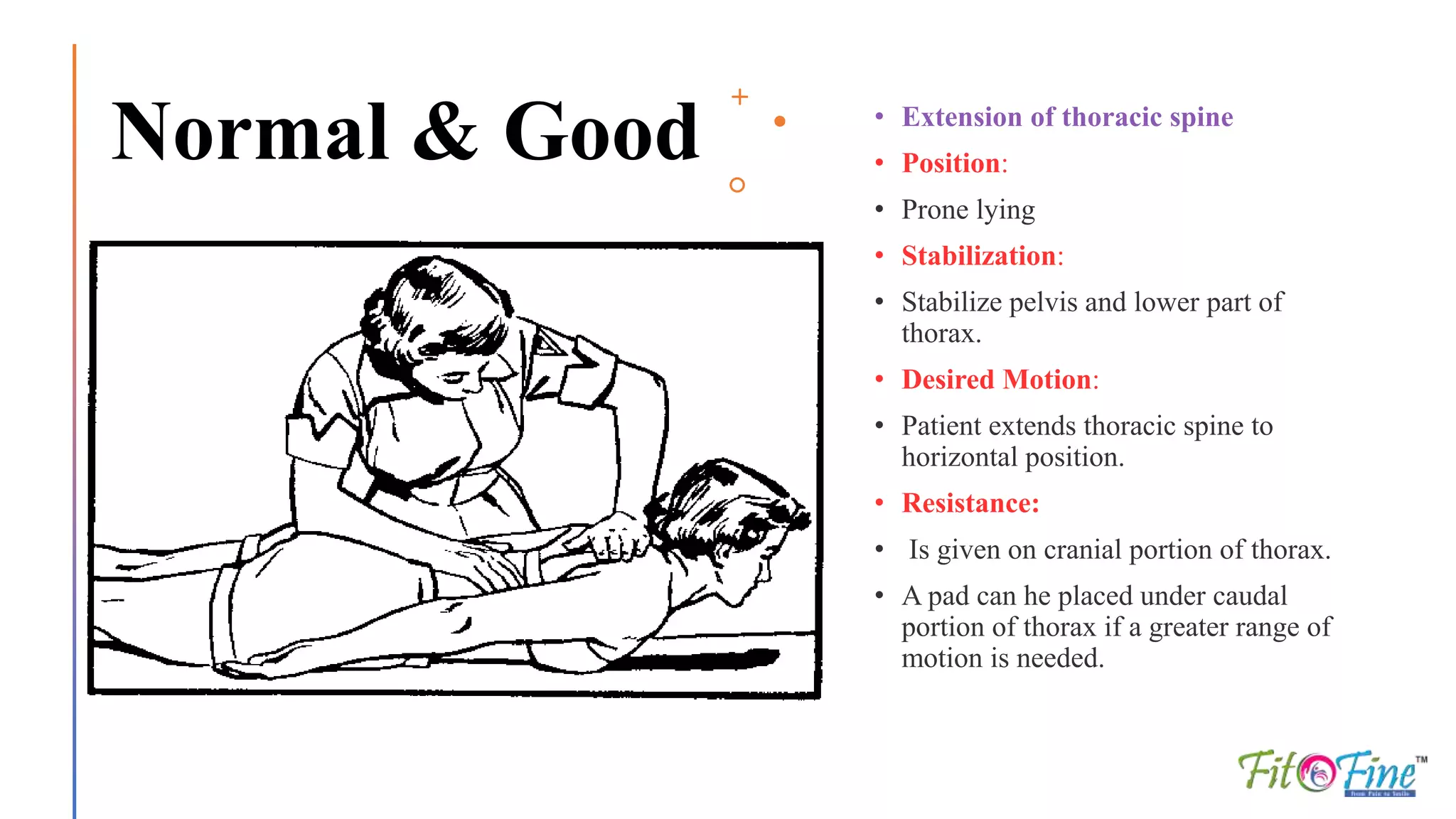
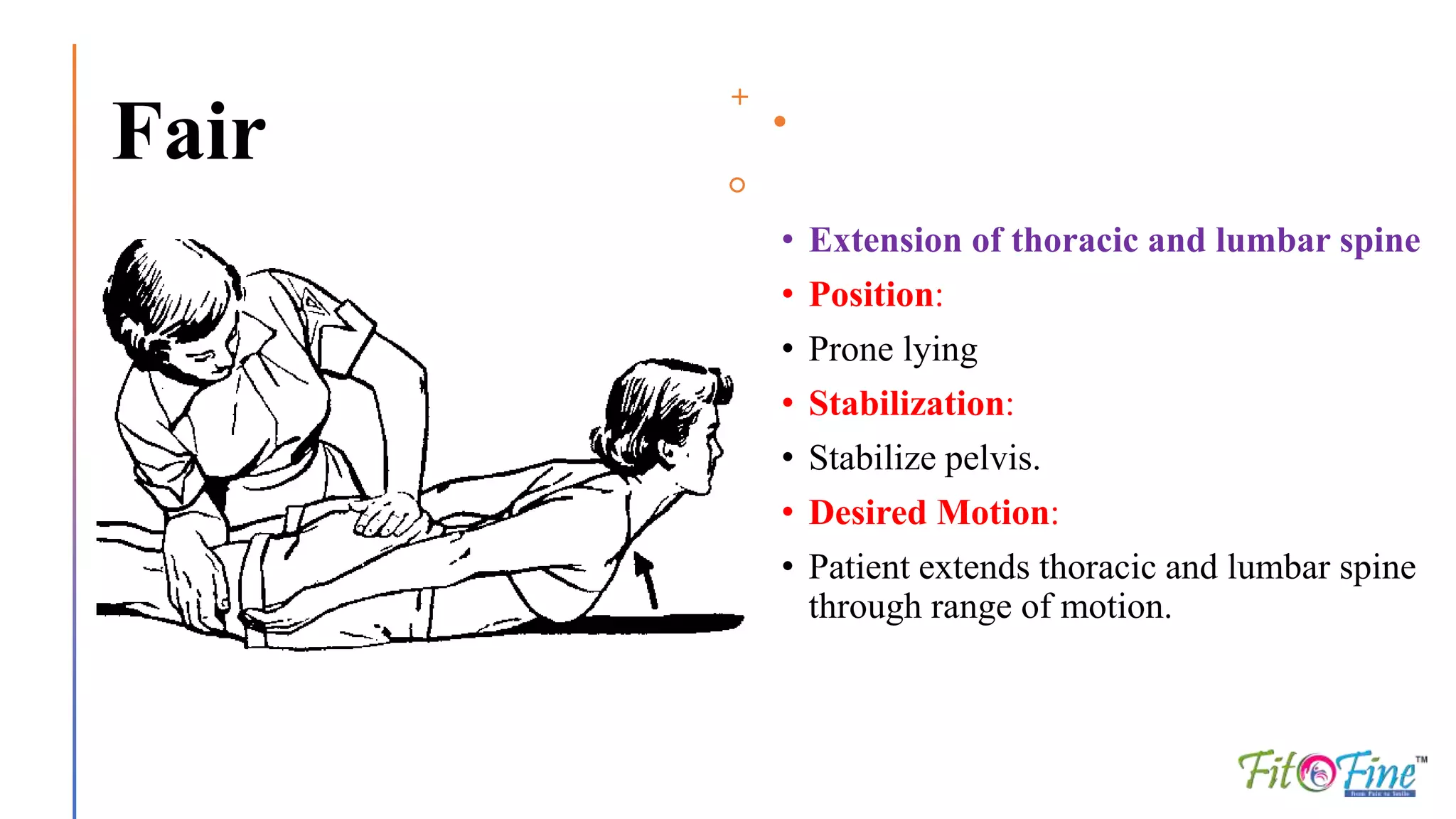

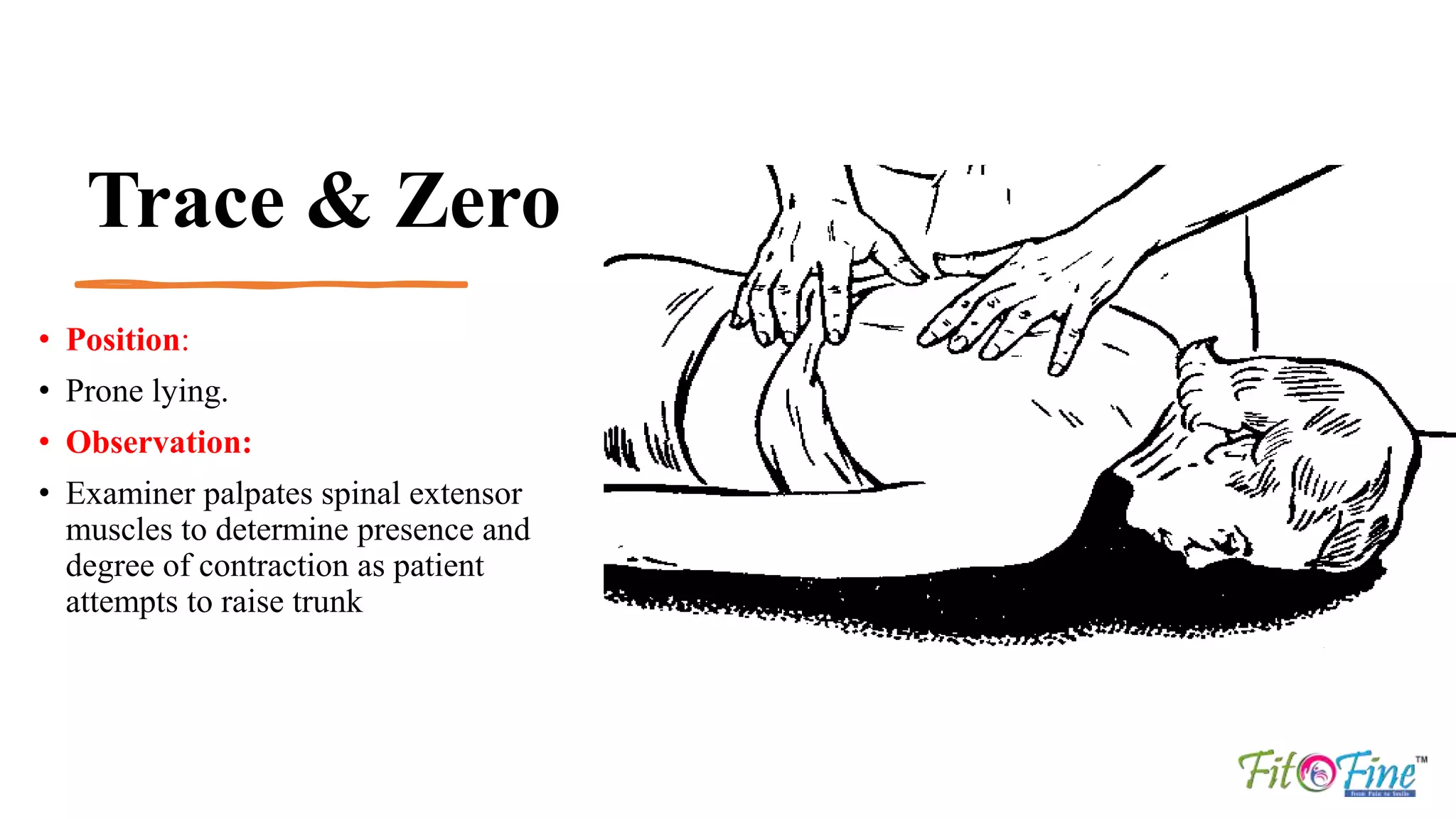

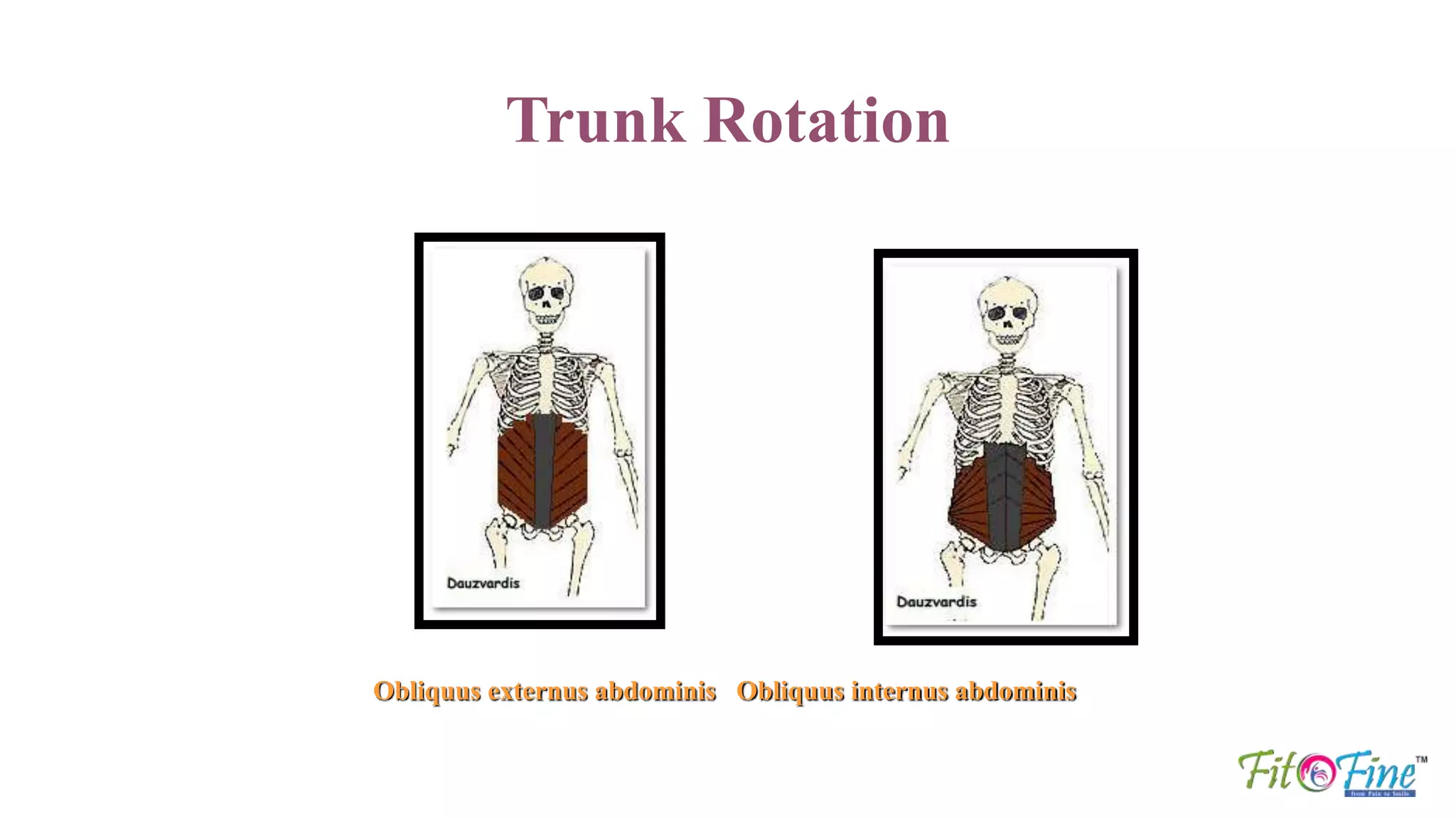
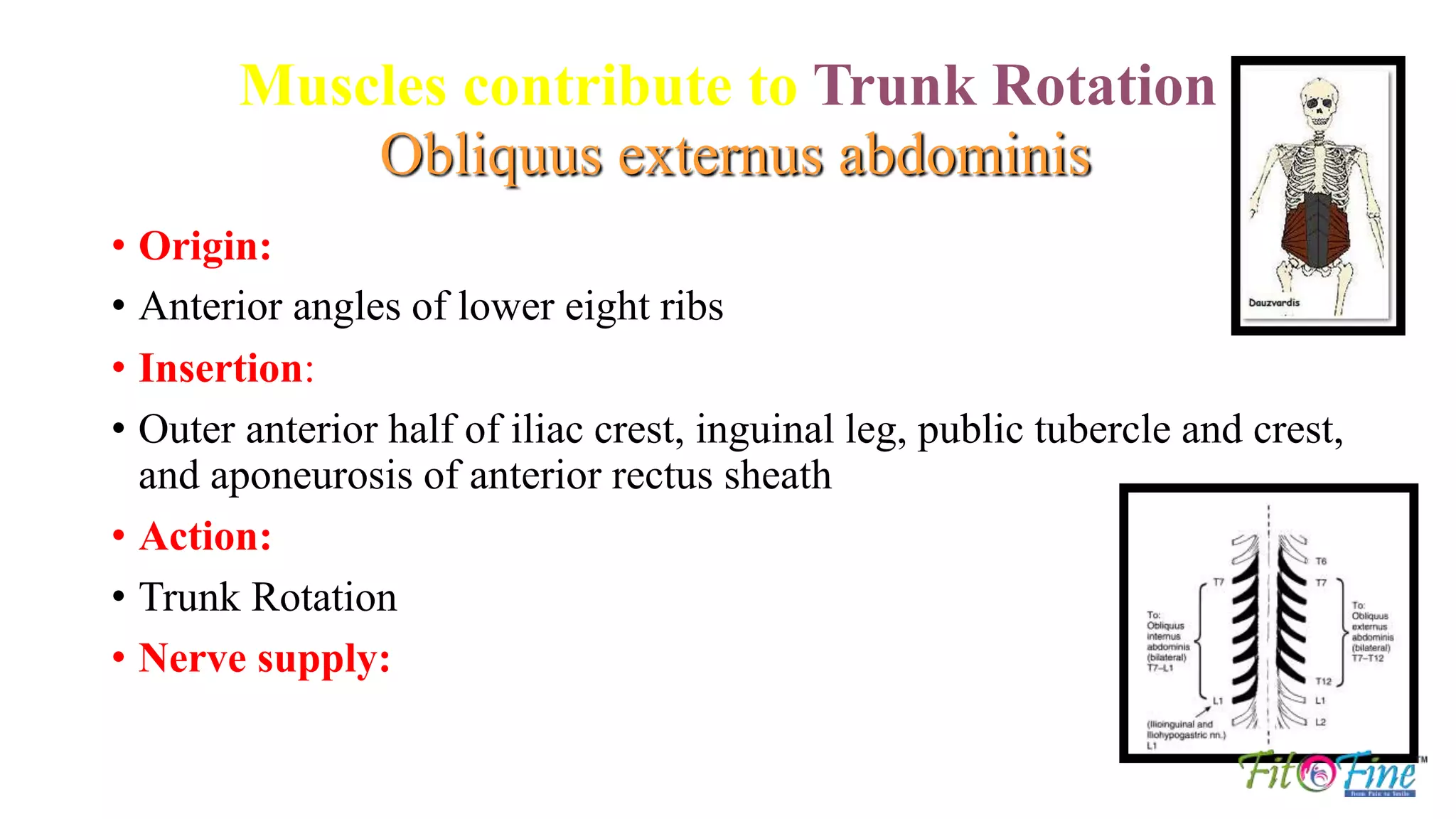
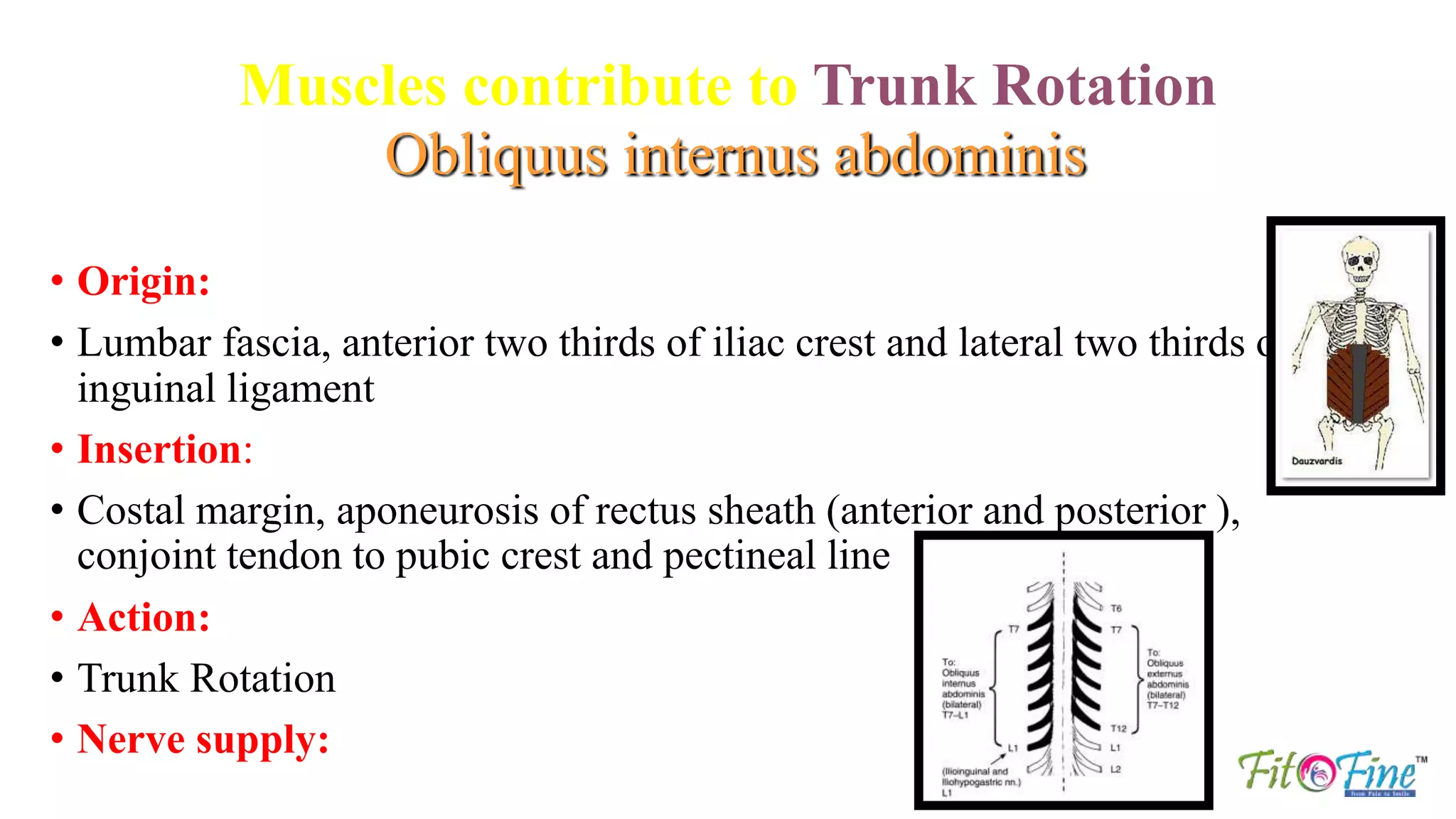
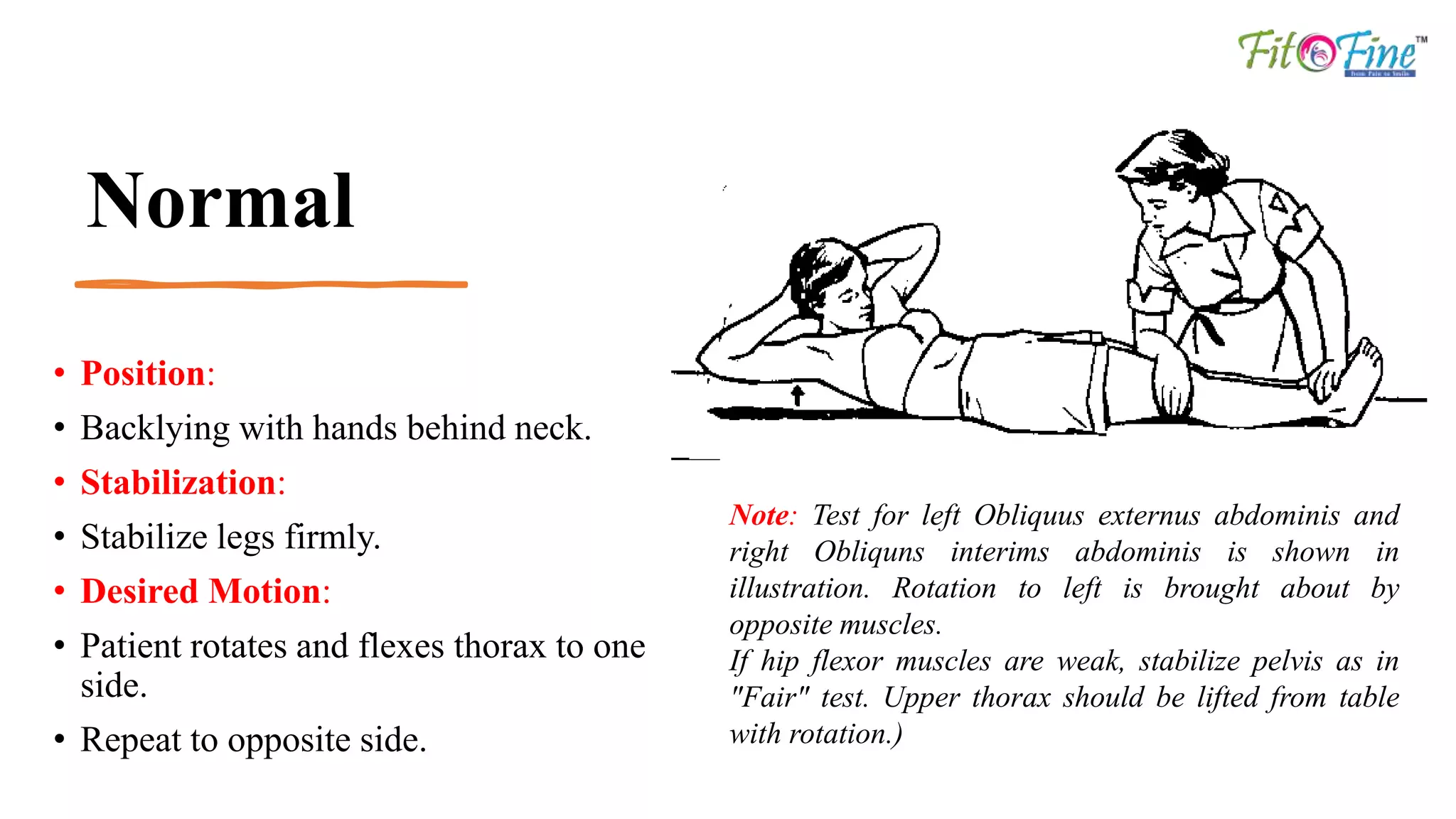
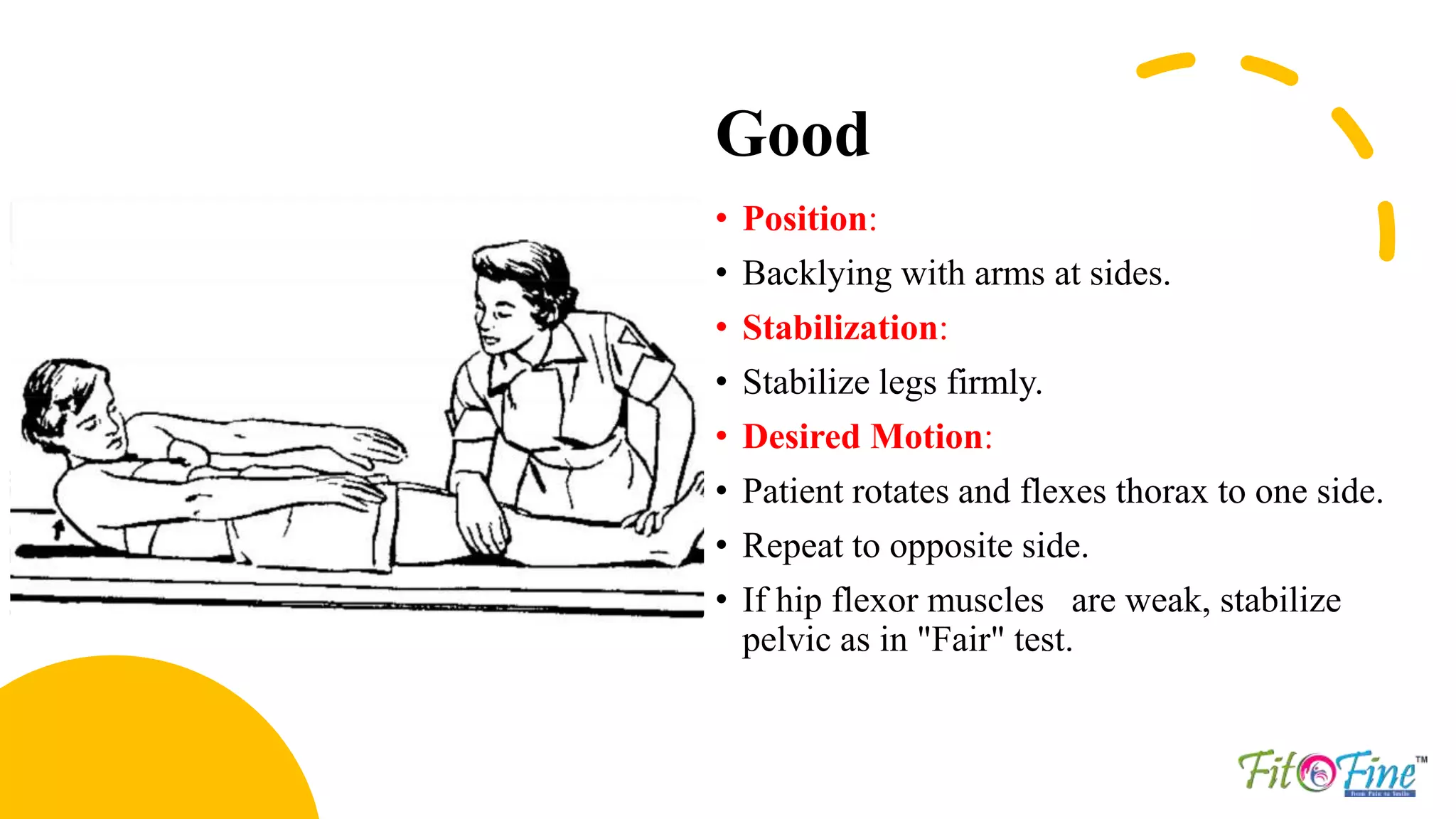
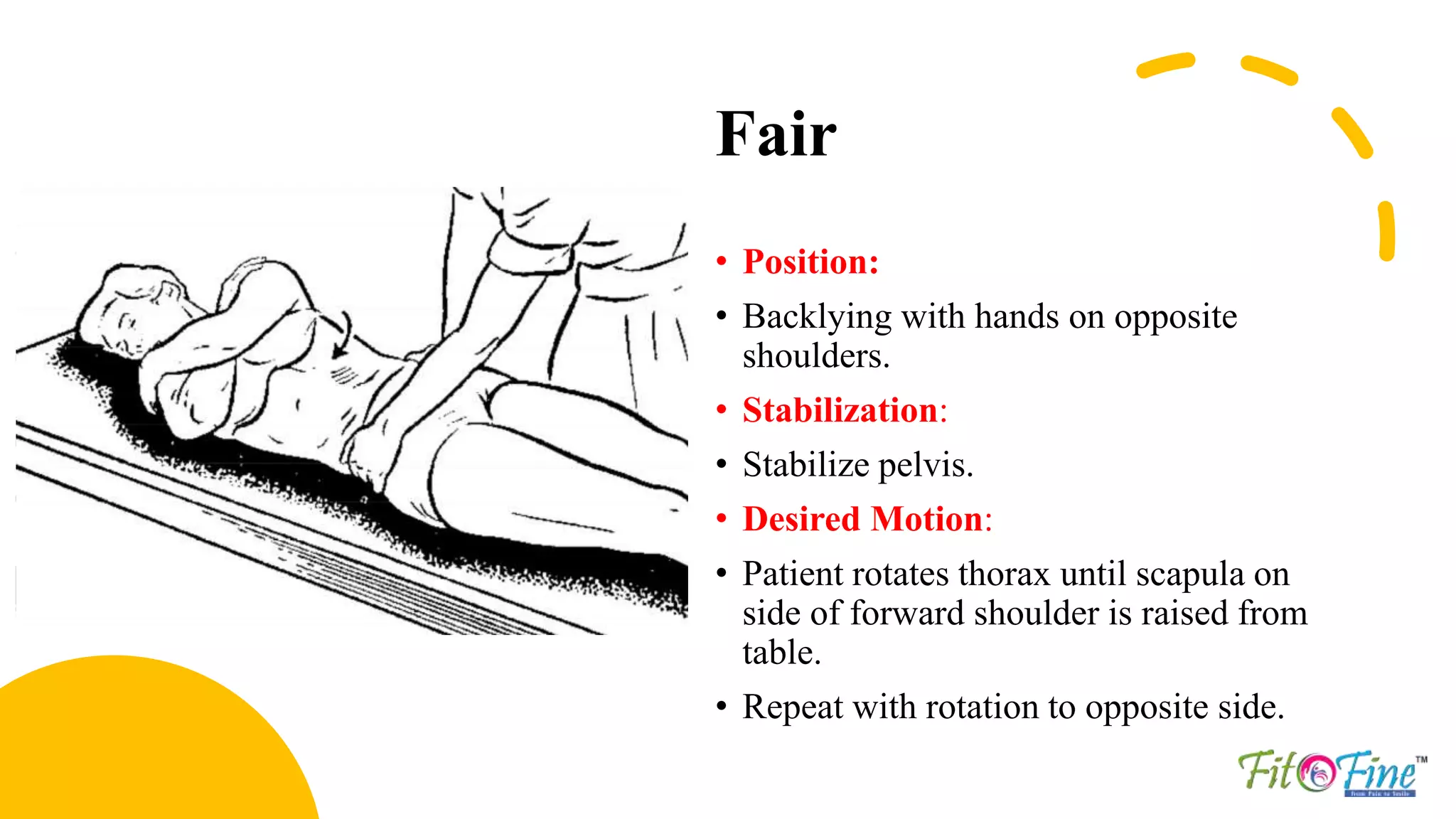
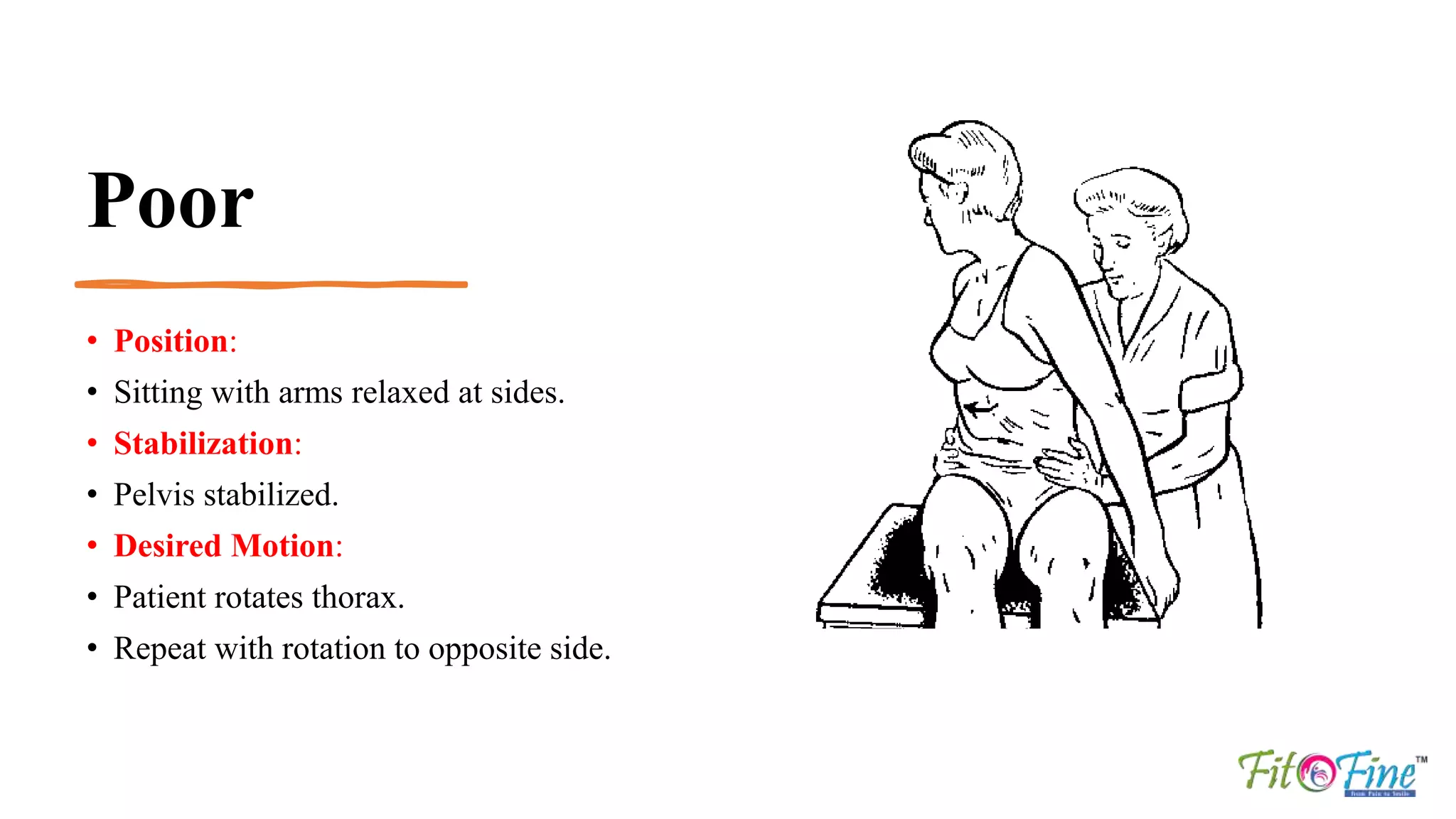
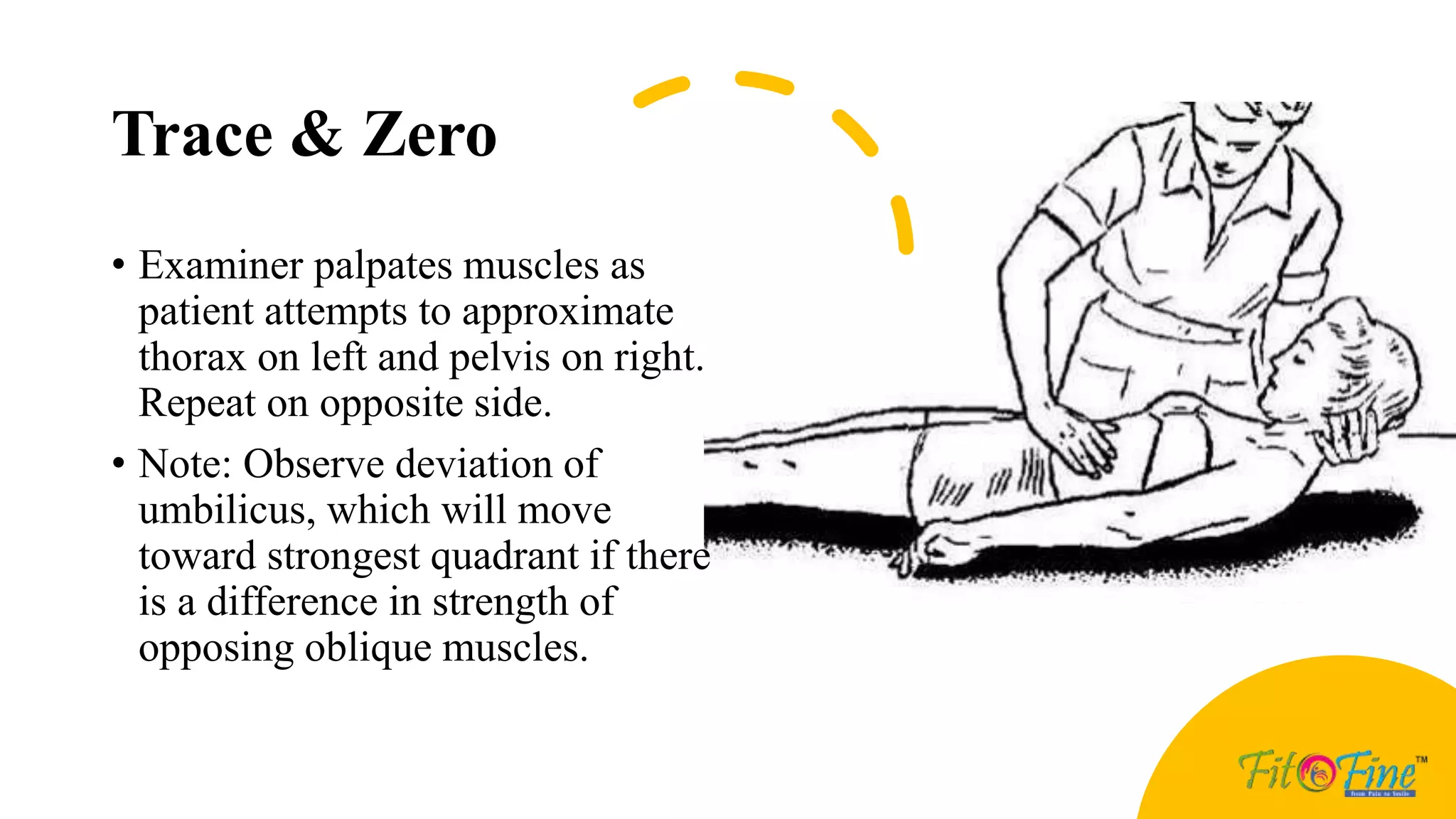

The document provides detailed descriptions of muscle testing techniques for trunk flexion, extension, and rotation, specifically focusing on the rectus abdominis and erector spinae muscles. It outlines different positions, stabilization methods, desired motions, and grading from normal to poor based on the patient's performance. Various factors that limit motion and testing methods are also noted, with references to established muscle testing techniques.























































































